

A Role for Oral Care in the Prevention of Hospital-Associated Pneumonia
As dental professionals, we are aware of the role of pathogenic and potentially pathogenic microorganisms present intraorally in oral and systemic infections. These microorganisms include ones that may present as a result of colonization from other sites (including the lungs). Oral care measures have been recommended to help reduce the microbial load, with the objective of reducing infections. Recent developments include a greater focus on the role of oral care in the prevention of non-ventilator hospital-associated pneumonia (NV-HAP) and ventilator-associated pneumonia (VAP), which together represent 22% of hospital-acquired infections (HAI).1Modi AR, Kovacs CS. Hospital-acquired and ventilator-associated pneumonia: Diagnosis, management, and prevention. Cleveland Clinic J Med 2020;87(10):633-9. doi: https://doi.org/10.3949/ccjm.87a.19117.,2Magill SS, O’Leary E, Janelle SJ et al; Emerging Infections Program Hospital Prevalence Survey Team. Changes in Prevalence of Health Care-Associated Infections in U.S. Hospitals. N Engl J Med 2018;379(18):1732-44. doi: 10.1056/NEJMoa1801550.
Types of pneumonia that develop in hospital
NV-HAP is new-onset pneumonia that develops in non-ventilated patients more than 48 hours after hospital admission and is the most frequently occurring HAI.1Modi AR, Kovacs CS. Hospital-acquired and ventilator-associated pneumonia: Diagnosis, management, and prevention. Cleveland Clinic J Med 2020;87(10):633-9. doi: https://doi.org/10.3949/ccjm.87a.19117.,2Magill SS, O’Leary E, Janelle SJ et al; Emerging Infections Program Hospital Prevalence Survey Team. Changes in Prevalence of Health Care-Associated Infections in U.S. Hospitals. N Engl J Med 2018;379(18):1732-44. doi: 10.1056/NEJMoa1801550. Sixty-five percent of pneumonia cases developing in hospital are attributable to NV-HAP, with an estimated incidence of 1.6% in admitted patients. VAP develops in the same timeframe in patients in ICU who have been intubated (and may or may not be by the time VAP develops).1Modi AR, Kovacs CS. Hospital-acquired and ventilator-associated pneumonia: Diagnosis, management, and prevention. Cleveland Clinic J Med 2020;87(10):633-9. doi: https://doi.org/10.3949/ccjm.87a.19117. Furthermore, VAP is estimated to occur in approximately 10% of patients who receive mechanical ventilation.
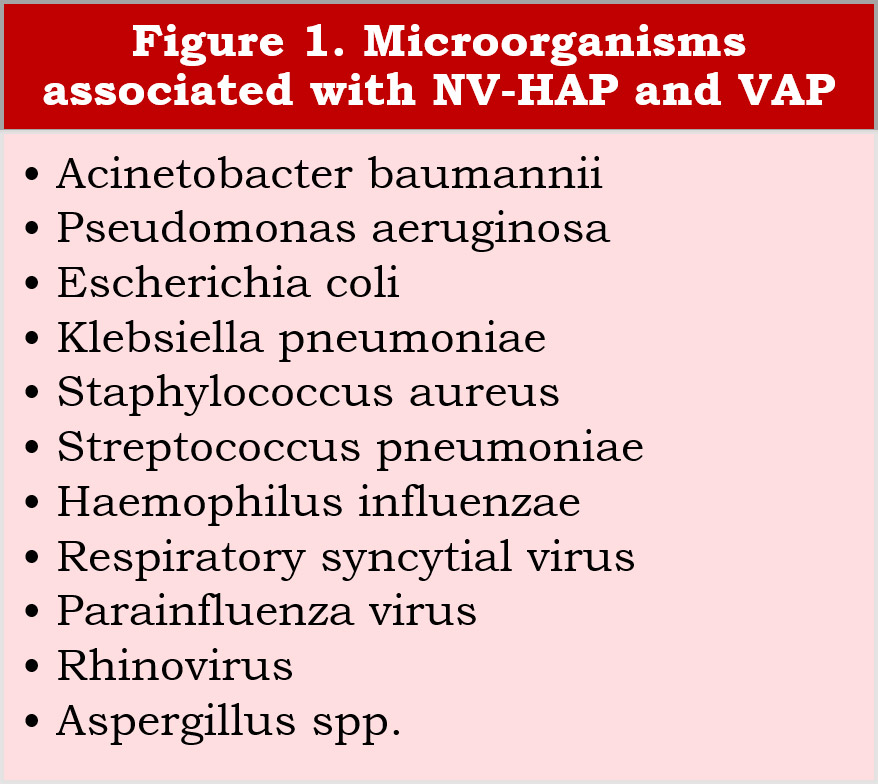
Microorganisms associated with NV-HAP and VAP
The microorganisms most frequently associated with NV-HAP and VAP include Acinetobacter baumannii, Pseudomonas aeruginosa, Escherichia coli (E.coli), Klebsiella pneumoniae, and Staphylococcus aureus.1Modi AR, Kovacs CS. Hospital-acquired and ventilator-associated pneumonia: Diagnosis, management, and prevention. Cleveland Clinic J Med 2020;87(10):633-9. doi: https://doi.org/10.3949/ccjm.87a.19117.,3Kalil AC, Metersky ML, Klompas M et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis 2016;63(5):e61-111. https://doi.org/10.1093/cid/ciw353.,4Abdalla JS, Albarrak M, Alhasawi A. et al. Narrative Review of the Epidemiology of Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia in Gulf Cooperation Council Countries. Infect Dis Ther 2023;12:1741-73. https://doi.org/10.1007/s40121-023-00834-w. Of further concern, for these microorganisms significant levels of multi-drug resistance are found globally.4Abdalla JS, Albarrak M, Alhasawi A. et al. Narrative Review of the Epidemiology of Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia in Gulf Cooperation Council Countries. Infect Dis Ther 2023;12:1741-73. https://doi.org/10.1007/s40121-023-00834-w. Other associated bacteria include Streptococcus pneumoniae and Haemophilus influenzae, while up to one-fifth of HAP and VAP infections are the result of colonization by viruses – notably, respiratory syncytial virus (RSV), parainfluenza virus, and rhinovirus.5Park DR. The microbiology of ventilator-associated pneumonia. Respir Care 2005;50(6):742-63.,6Sands KM, Twigg JA, Lewis MAO et al. Microbial profiling of dental plaque from mechanically ventilated patients. J Med Microbiol 2016;65(Pt 2):147-59.,7Hong HL, Hong SB, Ko GB et al. Viral infection is not uncommon in adult patients with severe hospital-acquired pneumonia. PLoS One 2014;9(4):e95865. doi:10.1371/journal.pone.0095865. Furthermore, fungi are a potential cause of VAP, including Aspergillus species.8Torres A, Martin-Loeches I. Invasive Pulmonary Aspergillosis in Ventilator-associated Pneumonia: The Hidden Enemy? Am J Respir Crit Care Med 2020;202(8):1071-3. doi: 10.1164/rccm.202006-2605ED.,9APIC Publishes Implementation Guide on NV-HAP. Arlington, VA, May 15, 2020. https://apic.org/apic-publishes-implementation-guide-on-nv-hap/. (Figure 1) Outbreaks of Candida auris in ICUs pose a further threat.4Abdalla JS, Albarrak M, Alhasawi A. et al. Narrative Review of the Epidemiology of Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia in Gulf Cooperation Council Countries. Infect Dis Ther 2023;12:1741-73. https://doi.org/10.1007/s40121-023-00834-w.
Risk Factors for NV-HAP and VAP
Aspiration of microorganisms is associated with NV-HAP. As such, dysphagia is a significant risk factor since it is associated with aspiration and is more prevalent in older adults.10Pusins JM, Ferguson C, Persaud AV. Oral Health and Aspiration Pneumonia. Today's Geriatric Med Vol 11(6):16. https://www.todaysgeriatricmedicine.com/archive/ND18p16.shtml. In the case of VAP, micro-aspiration can occur while the patient is being ventilated.11Gershonovitch R, Yarom N, Findler M. Preventing Ventilator-Associated Pneumonia in Intensive Care Unit by improved Oral Care: a Review of Randomized Control Trials. SN Compr Clin Med 2020;2(6):727-33. doi: 10.1007/s42399-020-00319-8. Other mechanisms by which microorganisms may invade the lungs in intubated patients include a gram-negative bacterial biofilm within the endotracheal tube, and secretions around the endotracheal tube.11Gershonovitch R, Yarom N, Findler M. Preventing Ventilator-Associated Pneumonia in Intensive Care Unit by improved Oral Care: a Review of Randomized Control Trials. SN Compr Clin Med 2020;2(6):727-33. doi: 10.1007/s42399-020-00319-8.
Risk factors for NV-HAP include being very young or very old, poor oral care (prior to and during hospitalization), impaired patient mobility, and the angle of the head of the bed.12Centers for Disease Control and Prevention. Healthcare-Associated Infections (HAIs). Oral Health in Healthcare Settings to Prevent Pneumonia Toolkit. https://www.cdc.gov/hai/prevent/Oral-Health-Toolkit.html. Additionally, older individuals are more likely to experience reduced self-cleansing of the oral environment as well as a reduced ability to masticate and swallow, and to have periodontal disease and poor oral hygiene with higher microbial loads.13Koichiro U. Preventing aspiration pneumonia by oral health care. JMAJ 2011;54(1):39-43. Patients who are immunocompromised, or who experience chronic respiratory disease or other chronic conditions, are also at increased risk for NV-HAP.13Koichiro U. Preventing aspiration pneumonia by oral health care. JMAJ 2011;54(1):39-43.,14Vignari M. Non-ventilator health care-associated pneumonia (NV-HAP): NV-HAP Risk Factors. Am J Infect Control 2020;48(5S):A10-13. doi: 10.1016/j.ajic.2020.03.010. Furthermore, medications that reduce gastric acid production, such as proton-pump inhibitors, enable colonization of the oropharynx and of endotracheal tubes by nosocomial pathogens, thereby presenting a risk for NV-HAP and VAP.1Modi AR, Kovacs CS. Hospital-acquired and ventilator-associated pneumonia: Diagnosis, management, and prevention. Cleveland Clinic J Med 2020;87(10):633-9. doi: https://doi.org/10.3949/ccjm.87a.19117. (Table 1)
| Table 1. Risk factors for NV-HAP |
|---|
| Dysphagia |
| Age (very young/very old) |
| Impaired mobility |
| Poor oral care |
| Compromised oral environment |
| Immunocompromised |
| Chronic respiratory disease/other chronic conditions |
| Angle of the head of the bed |
| Use of medications that reduce gastric acid production |
Risk factors for VAP include age and poor oral care prior to admission, neurological disorders, recent surgery, and insufficient provision of oral care by healthcare personnel during hospitalization.1Modi AR, Kovacs CS. Hospital-acquired and ventilator-associated pneumonia: Diagnosis, management, and prevention. Cleveland Clinic J Med 2020;87(10):633-9. doi: https://doi.org/10.3949/ccjm.87a.19117. In one study, it was concluded that the greatest risk factor for VAP was the duration of mechanical ventilation.15Chacko R, Rajan A, Lionel P. Oral decontamination techniques and ventilator-associated pneumonia. Br J Nurs 2017;26(11):594-9. doi: 10.12968/bjon.2017.26.11.594. In addition, patients with acute respiratory distress syndrome, cystic fibrosis, septic shock and extended hospitalization are considered at additional risk due to multi-drug resistant microorganisms.1Modi AR, Kovacs CS. Hospital-acquired and ventilator-associated pneumonia: Diagnosis, management, and prevention. Cleveland Clinic J Med 2020;87(10):633-9. doi: https://doi.org/10.3949/ccjm.87a.19117.
Oral Care Interventions to Help Prevent VAP
Reviews and individual studies have been conducted to evaluate the effect of oral care measures on the incidence of VAP. Other interventions aimed at preventing VAP and NV-HAP are beyond the scope of this article. In a recent systematic review and meta-analysis of 10 studies with more than 1200 patients mechanically ventilated for at least 48 hours, oral application of 0.12% CHX reduced the risk of VAP by 27%.16Cruz JC, Martins CK, Piassi JEV. Does chlorhexidine reduce the incidence of ventilator-associated pneumonia in ICU patients? A systematic review and meta-analysis. Med Intensiva (Engl Ed) 2023;47(8):437-444. doi: 10.1016/j.medine.2022.11.002. In a meta-analysis of 5 studies in patients admitted to ICU, the incidence of VAP decreased by more than half when oral care was provided.17de Araújo ECF, da Silva RO, Raymundo MLB et al. Does the presence of oral health teams influence the incidence of ventilator-associated pneumonia and mortality of patients in intensive care units? Systematic review. Spec Care Dentist 2023;43(4):452-63. doi: 10.1111/scd.12785. A systematic review and meta-analysis of 36 studies included more than 116,000 patients who were mechanically ventilated.18Martinez-Reviejo R, Tejada S, Jansson M et al. Prevention of ventilator-associated pneumonia through care bundles: A systematic review and meta-analysis. J Intensive Med. 2023;3(4):352-64. doi: 0.1016/j.jointm.2023.04.004. Approximately 72% of individuals received a care bundle that included oral care (and head-of-bed elevation). In comparison to those not receiving this care (the control group), the incidence of VAP decreased. In an evaluation of 18 RCT in another review, the researchers concluded that delivery of CHX as a component of provided oral care reduced the risk of VAP from 25% to ~19%.19Veitz-Keenan A, Ferraiolo DM. Oral care with chlorhexidine seems effective for reducing the incidence of ventilator-associated pneumonia. Evid Based Dent 2017;18(4):113-4. doi: 10.1038/sj.ebd.6401272.
Figure 2. Number of cases of VAP
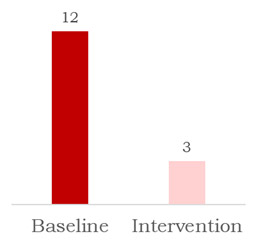
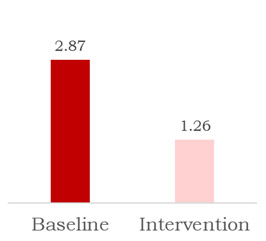
Figure 3. Cases per 1,000 ventilator days
In a two-state collaborative, 56 ICUs reported almost 70,000 patient days of ventilation.12Centers for Disease Control and Prevention. Healthcare-Associated Infections (HAIs). Oral Health in Healthcare Settings to Prevent Pneumonia Toolkit. https://www.cdc.gov/hai/prevent/Oral-Health-Toolkit.html. VAP was significantly reduced when oral care was provided, with the incidence of VAP decreasing from 3.15 to 1.56 per 1,000 ventilator days.
In another study, the incidence rate for VAP was reduced more by brushing four times daily compared to twice daily.20Haghighat S, Mahjobipoor H, Gavarti SG. Comparative study of the effect of three oral care protocols on ventilator-associated pneumonia in critically ill patients: A clinical trial. Iran J Nurs Midwifery Res 2022;27:99-105. In contrast, in a review of 8 studies, for 6 of these no significant differences in VAP incidence were found for test and control groups.12Centers for Disease Control and Prevention. Healthcare-Associated Infections (HAIs). Oral Health in Healthcare Settings to Prevent Pneumonia Toolkit. https://www.cdc.gov/hai/prevent/Oral-Health-Toolkit.html. Similarly, no improvements were found in a clinical study with 80 patients.21Atashi V, Yousefi H, Mahjobipoor H et al. Effect of oral care program on prevention of ventilator associated pneumonia in intensive care unit patients: A randomized controlled trial. Iranian J Nursing Midwifery Res 2018;23:486-90.
The outcomes of standardized, evidence-based oral care protocols were evaluated in a retrospective study with approximately 400 patients who were ventilated, at-risk, or short-term care trauma (nonventilated) patients.22C, Medei MK, Wood B, Schutte D. A Nurse-Driven Oral Care Protocol to Reduce Hospital-Acquired Pneumonia. Am J Nurs 2019;119(2):44-51. doi: 10.1097/01.NAJ.0000553204.21342.01. Individuals receiving mechanical ventilation or at-risk received care with a new suction toothbrush kit. The incidence of VAP was measured in identical seven-month periods in each of two years. There were 56 ventilator-associated events with 12 and 3 cases of VAP, respectively, in the baseline and intervention groups. (Figure 2) Infection rates were 2.87 and 1.26 cases per 1,000 ventilator days, respectively, for the two groups. (Figure 3) In several studies, however, no evidence was found that toothbrushing was beneficial over and above the use of an antimicrobial rinse/gel, including in two studies where the oral care protocol involved suctioning.15Chacko R, Rajan A, Lionel P. Oral decontamination techniques and ventilator-associated pneumonia. Br J Nurs 2017;26(11):594-9. doi: 10.12968/bjon.2017.26.11.594.,19Veitz-Keenan A, Ferraiolo DM. Oral care with chlorhexidine seems effective for reducing the incidence of ventilator-associated pneumonia. Evid Based Dent 2017;18(4):113-4. doi: 10.1038/sj.ebd.6401272. ,23Pobo A, Lisboa T, Rodriguez A et al. A randomized trial of dental brushing for preventing ventilator associated pneumonia. Chest 2009;136(2):433-9.,24de Lacerda Vidal CF, Vidal AK, Monteiro JG Jr et al. Impact of hygiene involving toothbrushing versus chlorhexidine in the prevention of ventilator associated pneumonia: a randomized study. BMC Infect Dis 2017;17(1):112.,25Lorente L, Lecuona M, Jiménez A et al. Ventilator-associated pneumonia with or without toothbrushing: a randomized controlled trial. Eur J Clin Microbiol Infect Dis 2012;31(10):2621-9.,26de Camargo L, da Silva SN, Chambrone L. Efficacy of toothbrushing procedures performed in intensive care units in reducing the risk of ventilator-associated pneumonia: A systematic review. J Periodontal Res 2019;54(6):601-11. doi: 10.1111/jre.12668.
Microbial contamination of the oropharynx decreases when professional oral care including mouth swabbing with 0.12% CHX is provided.27Kes D, Yildirim TA, Kuru C et al. Effect of 0.12% Chlorhexidine Use for Oral Care on Ventilator-Associated Respiratory Infections: A Randomized Controlled Trial. J Trauma Nurs 2021;28(4):228-34. doi:10.1097/JTN.0000000000000590.,28Choi M-I, Han S-Y, Jeon H-S et al. The influence of professional oral hygiene care on reducing ventilator-associated pneumonia in trauma intensive care unit patients. Br Dent J 2022;232(4):253-9. doi: 10.1038/s41415-022-3986-3. In one study, samples were obtained from oral mucosa and dental plaque when patients were admitted to an ICU as well as on days 3,5,7 and 10.29Tuon FF, Gavrilko O, de Almeida S et al. Prospective, randomised, controlled study evaluating early modification of oral microbiota following admission to the intensive care unit and oral hygiene with chlorhexidine. J Glob Antimicrob Resist 2017:8:159-63. doi: 10.1016/j.jgar.2016.12.007. The group receiving treatment with 2% CHX following admission had a lower incidence of MRSA compared to the control group. Significant reductions in colony-forming units were found for Staphylococcus aureus and Klebsiella pneumoniae. In addition, a positive dose-response was found in a study evaluating decontamination with 0.2% or 2% CHX.30Zand F, Zahed L, Mansouri P et al. The effects of oral rinse with 0.2% and 2% chlorhexidine on oropharyngeal colonization and ventilator associated pneumonia in adults' intensive care units. J Crit Care 2017;40:318-22.
Oral Care Interventions to Help Prevent NV-HAP
Several NV-HAP Prevention Programs that incorporate standardized oral care protocols have demonstrated positive results in reducing the incidence of NV-HAP. In a veterans hospital, over a 19-month period starting in 2016, the incidence of NV-HAP was reduced by 92% and healthcare cost savings were estimated at $2.84 million.31Munro S, Baker D. Reducing missed oral care opportunities to prevent non-ventilator associated hospital acquired pneumonia at the Department of Veterans Affairs. Appl Nurs Res 2018;44:48-53. doi: 10.1016/j.apnr.2018.09.004. In another multi-center program, the incidence of NV-HAP decreased by 40 to 60% across sites and the 1-year direct healthcare cost savings per case prevented has been estimated at $100,000 (2016).32Munro S, Haile-Mariam A, Greenwell C et al. Implementation and Dissemination of a Department of Veterans Affairs Oral Care Initiative to Prevent Hospital-Acquired Pneumonia Among Nonventilated Patients. Nurs Adm Q 2018;42(4):363-72. doi:1097/NAQ.0000000000000308.,33VA Diffusion Marketplace. Hospital acquired pneumonia prevention by engaging nurses (HAPPEN). https://marketplace.va.gov/innovations/project-happen. In a third program, over 12 months, the incidence of NV-HAP decreased by 85% and 56%, respectively, for medical and surgical units.34Giuliano KK, Penoyer D, Middleton A, Baker D. Original Research: Oral Care as Prevention for Nonventilator Hospital-Acquired Pneumonia: A Four-Unit Cluster Randomized Study. Am J Nurs 2021;121(6):24-33. doi: 10.1097/01.NAJ.0000753468.99321.93. In one study, short-term care patients with trauma received an oral care kit consisting of an ergonomically designed toothbrush, toothpaste, and an alcohol-free antiseptic mouthwash.24de Lacerda Vidal CF, Vidal AK, Monteiro JG Jr et al. Impact of hygiene involving toothbrushing versus chlorhexidine in the prevention of ventilator associated pneumonia: a randomized study. BMC Infect Dis 2017;17(1):112. The incidence of NV-HAP was determined in identical seven-month periods in each of two years. The number of cases of NV-HAP dropped to 26 in the intervention group, compared to 52 cases in the baseline group.
The CDC Toolkit for Oral Care to prevent NV-HAP
Most recently, the CDC developed a toolkit containing guidance and recommendations to help develop oral care in hospital settings to prevent NV-HAP.12Centers for Disease Control and Prevention. Healthcare-Associated Infections (HAIs). Oral Health in Healthcare Settings to Prevent Pneumonia Toolkit. https://www.cdc.gov/hai/prevent/Oral-Health-Toolkit.html. It is recommended that an oral health assessment be performed and risk factors for NV-HAP identified at the time of the patient’s hospital admission. Consideration of physical limitations, special needs, ability to perform oral care, supplies needed, beliefs and dental history. Other recommendations include the following:12Centers for Disease Control and Prevention. Healthcare-Associated Infections (HAIs). Oral Health in Healthcare Settings to Prevent Pneumonia Toolkit. https://www.cdc.gov/hai/prevent/Oral-Health-Toolkit.html.
- Develop a plan for the patient’s oral hygiene (self-care).
- Provide oral hygiene instructions.
- Provide oral care products including a toothbrush, toothpaste, (alcohol-free) mouthrinse, and other items as needed (e.g., moisturizing agents).
- When medical personnel provide oral care for patients, use a toothbrush attached to suction (‘suctioning toothbrush’) to remove fluid and debris prior to brushing and after brushing, and wipe a mouth swab saturated with an antimicrobial rinse over the teeth and oral mucosa.
The toolkit provides a list of resources with links for oral health history forms, oral health assessment tools, information on providing oral care assistance to support patients as needed, and staff training for non-dental healthcare professionals. Examples of oral care procedures for patient self-care and assisted care are included, as well as information for patients on performing oral hygiene to prevent NV-HAP. Staff training on oral care has been shown to improve the compliance of healthcare personnel providing oral care. In one study, compliance with the provision of daily oral care by nursing staff increased to 92.8% from 29.6% after the educational intervention.35Sánchez M, Orozco LA, Barrios FA, Suárez OF. Impact of an Educational Intervention Aimed at Nursing Staff on Oral Hygiene Care on the Incidence of Ventilator-Associated Pneumonia in Adults Ventilated in Intensive Care Unit. Invest Educ Enferm 2021;39(3):e06. doi: https://doi.org/10.17533/udea.iee.v39n3e06. Additional approaches are also being researched, including the use of probiotics containing Lactobacillus, Bifidobacterium, and Streptococcus spp.36Mahmoodpoor A, Hamishehkar H, Asghari R et al. Effect of a Probiotic Preparation on Ventilator-Associated Pneumonia in Critically Ill Patients Admitted to the Intensive Care Unit: A Prospective Double-Blind Randomized Controlled Trial. Nutr Clin Pract 2019;34(1):156-62. doi: 10.1002/ncp.10191. In one pilot intervention, their use for two weeks resulted in significant reductions in the incidence of VAP compared to the control group.36Mahmoodpoor A, Hamishehkar H, Asghari R et al. Effect of a Probiotic Preparation on Ventilator-Associated Pneumonia in Critically Ill Patients Admitted to the Intensive Care Unit: A Prospective Double-Blind Randomized Controlled Trial. Nutr Clin Pract 2019;34(1):156-62. doi: 10.1002/ncp.10191.
Medical-Dental Collaboration
It is recommended that healthcare facilities develop written protocols for oral care for the prevention of NV-HAP, a multi-disciplinary team including medical personnel, dental professionals and clinical education teams, and share best practices.12Centers for Disease Control and Prevention. Healthcare-Associated Infections (HAIs). Oral Health in Healthcare Settings to Prevent Pneumonia Toolkit. https://www.cdc.gov/hai/prevent/Oral-Health-Toolkit.html. In the medical setting, patients should be encouraged to visit their dentist prior to planned hospitalizations to receive preventive care and other needed dental care, and if they do not have a dental home to establish one. Dental professionals already educate their patients on oral hygiene and the risks of poor oral health for systemic health, and NV-HAP and VAP are two situations where risk is directly enhanced during hospitalization. The dental team can help educate medical personnel on oral care, and the recent CDC publication on the oral care toolkit provides many resources and collaborate further with their medical colleagues in helping to prevent NV-HAP and VAP.
Conclusions
NV-HAP and VAP together are the most common HAIs, result in morbidity and mortality for patients, with mortality rates of 15 to 30% and an estimated 13%, respectively.9APIC Publishes Implementation Guide on NV-HAP. Arlington, VA, May 15, 2020. https://apic.org/apic-publishes-implementation-guide-on-nv-hap/.,12Centers for Disease Control and Prevention. Healthcare-Associated Infections (HAIs). Oral Health in Healthcare Settings to Prevent Pneumonia Toolkit. https://www.cdc.gov/hai/prevent/Oral-Health-Toolkit.html.,37Melsen WG, Rovers MM, Groenwold RH et al. Attributable mortality of ventilator-associated pneumonia: a meta-analysis of individual patient data from randomised prevention studies. Lancet Infect Dis 2013;13:665-71. doi:10.1016/S1473-3099(13)70081-1. In addition, longer-duration ICU care is associated with VAP. However, NV-HAP and VAP are preventable. Given the increase in multi-drug resistant microorganisms and the resulting difficulty in treating infections, the need for prevention is critical. Furthermore, reduced use of antibiotics is achieved when infection is prevented, as a further aspect of antibiotic stewardship. More research on outcomes and best practices for oral care protocols for the prevention of NV-HAP and VAP is needed, while recent study outcomes with respect to oral care protocols are encouraging, in particular for NV-HAP. Both types of hospital-associated pneumonia discussed in this article are preventable, and there is an opportunity through medical and dental collaboration to reduce patient suffering, and the costs of the associated healthcare burden.
References
- 1.Modi AR, Kovacs CS. Hospital-acquired and ventilator-associated pneumonia: Diagnosis, management, and prevention. Cleveland Clinic J Med 2020;87(10):633-9. doi: https://doi.org/10.3949/ccjm.87a.19117.
- 2.Magill SS, O’Leary E, Janelle SJ et al; Emerging Infections Program Hospital Prevalence Survey Team. Changes in Prevalence of Health Care-Associated Infections in U.S. Hospitals. N Engl J Med 2018;379(18):1732-44. doi: 10.1056/NEJMoa1801550.
- 3.Kalil AC, Metersky ML, Klompas M et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis 2016;63(5):e61-111. https://doi.org/10.1093/cid/ciw353.
- 4.Abdalla JS, Albarrak M, Alhasawi A. et al. Narrative Review of the Epidemiology of Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia in Gulf Cooperation Council Countries. Infect Dis Ther 2023;12:1741-73. https://doi.org/10.1007/s40121-023-00834-w.
- 5.Park DR. The microbiology of ventilator-associated pneumonia. Respir Care 2005;50(6):742-63.
- 6.Sands KM, Twigg JA, Lewis MAO et al. Microbial profiling of dental plaque from mechanically ventilated patients. J Med Microbiol 2016;65(Pt 2):147-59.
- 7.Hong HL, Hong SB, Ko GB et al. Viral infection is not uncommon in adult patients with severe hospital-acquired pneumonia. PLoS One 2014;9(4):e95865. doi:10.1371/journal.pone.0095865.
- 8.Torres A, Martin-Loeches I. Invasive Pulmonary Aspergillosis in Ventilator-associated Pneumonia: The Hidden Enemy? Am J Respir Crit Care Med 2020;202(8):1071-3. doi: 10.1164/rccm.202006-2605ED.
- 9.APIC Publishes Implementation Guide on NV-HAP. Arlington, VA, May 15, 2020. https://apic.org/apic-publishes-implementation-guide-on-nv-hap/.
- 10.Pusins JM, Ferguson C, Persaud AV. Oral Health and Aspiration Pneumonia. Today's Geriatric Med Vol 11(6):16. https://www.todaysgeriatricmedicine.com/archive/ND18p16.shtml.
- 11.Gershonovitch R, Yarom N, Findler M. Preventing Ventilator-Associated Pneumonia in Intensive Care Unit by improved Oral Care: a Review of Randomized Control Trials. SN Compr Clin Med 2020;2(6):727-33. doi: 10.1007/s42399-020-00319-8.
- 12.Centers for Disease Control and Prevention. Healthcare-Associated Infections (HAIs). Oral Health in Healthcare Settings to Prevent Pneumonia Toolkit. https://www.cdc.gov/hai/prevent/Oral-Health-Toolkit.html.
- 13.Koichiro U. Preventing aspiration pneumonia by oral health care. JMAJ 2011;54(1):39-43.
- 14.Vignari M. Non-ventilator health care-associated pneumonia (NV-HAP): NV-HAP Risk Factors. Am J Infect Control 2020;48(5S):A10-13. doi: 10.1016/j.ajic.2020.03.010.
- 15.Chacko R, Rajan A, Lionel P. Oral decontamination techniques and ventilator-associated pneumonia. Br J Nurs 2017;26(11):594-9. doi: 10.12968/bjon.2017.26.11.594.
- 16.Cruz JC, Martins CK, Piassi JEV. Does chlorhexidine reduce the incidence of ventilator-associated pneumonia in ICU patients? A systematic review and meta-analysis. Med Intensiva (Engl Ed) 2023;47(8):437-444. doi: 10.1016/j.medine.2022.11.002.
- 17.de Araújo ECF, da Silva RO, Raymundo MLB et al. Does the presence of oral health teams influence the incidence of ventilator-associated pneumonia and mortality of patients in intensive care units? Systematic review. Spec Care Dentist 2023;43(4):452-63. doi: 10.1111/scd.12785.
- 18.Martinez-Reviejo R, Tejada S, Jansson M et al. Prevention of ventilator-associated pneumonia through care bundles: A systematic review and meta-analysis. J Intensive Med. 2023;3(4):352-64. doi: 0.1016/j.jointm.2023.04.004.
- 19.Veitz-Keenan A, Ferraiolo DM. Oral care with chlorhexidine seems effective for reducing the incidence of ventilator-associated pneumonia. Evid Based Dent 2017;18(4):113-4. doi: 10.1038/sj.ebd.6401272.
- 20.Haghighat S, Mahjobipoor H, Gavarti SG. Comparative study of the effect of three oral care protocols on ventilator-associated pneumonia in critically ill patients: A clinical trial. Iran J Nurs Midwifery Res 2022;27:99-105.
- 21.Atashi V, Yousefi H, Mahjobipoor H et al. Effect of oral care program on prevention of ventilator associated pneumonia in intensive care unit patients: A randomized controlled trial. Iranian J Nursing Midwifery Res 2018;23:486-90.
- 22.C, Medei MK, Wood B, Schutte D. A Nurse-Driven Oral Care Protocol to Reduce Hospital-Acquired Pneumonia. Am J Nurs 2019;119(2):44-51. doi: 10.1097/01.NAJ.0000553204.21342.01.
- 23.Pobo A, Lisboa T, Rodriguez A et al. A randomized trial of dental brushing for preventing ventilator associated pneumonia. Chest 2009;136(2):433-9.
- 24.de Lacerda Vidal CF, Vidal AK, Monteiro JG Jr et al. Impact of hygiene involving toothbrushing versus chlorhexidine in the prevention of ventilator associated pneumonia: a randomized study. BMC Infect Dis 2017;17(1):112.
- 25.Lorente L, Lecuona M, Jiménez A et al. Ventilator-associated pneumonia with or without toothbrushing: a randomized controlled trial. Eur J Clin Microbiol Infect Dis 2012;31(10):2621-9.
- 26.de Camargo L, da Silva SN, Chambrone L. Efficacy of toothbrushing procedures performed in intensive care units in reducing the risk of ventilator-associated pneumonia: A systematic review. J Periodontal Res 2019;54(6):601-11. doi: 10.1111/jre.12668.
- 27.Kes D, Yildirim TA, Kuru C et al. Effect of 0.12% Chlorhexidine Use for Oral Care on Ventilator-Associated Respiratory Infections: A Randomized Controlled Trial. J Trauma Nurs 2021;28(4):228-34. doi:10.1097/JTN.0000000000000590.
- 28.Choi M-I, Han S-Y, Jeon H-S et al. The influence of professional oral hygiene care on reducing ventilator-associated pneumonia in trauma intensive care unit patients. Br Dent J 2022;232(4):253-9. doi: 10.1038/s41415-022-3986-3.
- 29.Tuon FF, Gavrilko O, de Almeida S et al. Prospective, randomised, controlled study evaluating early modification of oral microbiota following admission to the intensive care unit and oral hygiene with chlorhexidine. J Glob Antimicrob Resist 2017:8:159-63. doi: 10.1016/j.jgar.2016.12.007.
- 30.Zand F, Zahed L, Mansouri P et al. The effects of oral rinse with 0.2% and 2% chlorhexidine on oropharyngeal colonization and ventilator associated pneumonia in adults' intensive care units. J Crit Care 2017;40:318-22.
- 31.Munro S, Baker D. Reducing missed oral care opportunities to prevent non-ventilator associated hospital acquired pneumonia at the Department of Veterans Affairs. Appl Nurs Res 2018;44:48-53. doi: 10.1016/j.apnr.2018.09.004.
- 32.Munro S, Haile-Mariam A, Greenwell C et al. Implementation and Dissemination of a Department of Veterans Affairs Oral Care Initiative to Prevent Hospital-Acquired Pneumonia Among Nonventilated Patients. Nurs Adm Q 2018;42(4):363-72. doi:1097/NAQ.0000000000000308.
- 33.VA Diffusion Marketplace. Hospital acquired pneumonia prevention by engaging nurses (HAPPEN). https://marketplace.va.gov/innovations/project-happen.
- 34.Giuliano KK, Penoyer D, Middleton A, Baker D. Original Research: Oral Care as Prevention for Nonventilator Hospital-Acquired Pneumonia: A Four-Unit Cluster Randomized Study. Am J Nurs 2021;121(6):24-33. doi: 10.1097/01.NAJ.0000753468.99321.93.
- 35.Sánchez M, Orozco LA, Barrios FA, Suárez OF. Impact of an Educational Intervention Aimed at Nursing Staff on Oral Hygiene Care on the Incidence of Ventilator-Associated Pneumonia in Adults Ventilated in Intensive Care Unit. Invest Educ Enferm 2021;39(3):e06. doi: https://doi.org/10.17533/udea.iee.v39n3e06.
- 36.Mahmoodpoor A, Hamishehkar H, Asghari R et al. Effect of a Probiotic Preparation on Ventilator-Associated Pneumonia in Critically Ill Patients Admitted to the Intensive Care Unit: A Prospective Double-Blind Randomized Controlled Trial. Nutr Clin Pract 2019;34(1):156-62. doi: 10.1002/ncp.10191.
- 37.Melsen WG, Rovers MM, Groenwold RH et al. Attributable mortality of ventilator-associated pneumonia: a meta-analysis of individual patient data from randomised prevention studies. Lancet Infect Dis 2013;13:665-71. doi:10.1016/S1473-3099(13)70081-1.