

Dental Professionals: Identifying and Reporting Suspected Child Abuse
Child abuse refers to the physical, emotional (psychological) and/or sexual abuse of a child.1Han H, Lees AB, Morse Z, Koziol-McLain J. Child abuse knowledge and attitudes among dental and oral health therapists in Aotearoa New Zealand: a cross-sectional study. BMC Health Serv Res 2022;22(1):1504. doi: 10.1186/s12913-022-08907-1.,2Centers for Disease Control and Prevention. Violence Prevention. Fast Facts: Preventing Child Abuse & Neglect. https://www.cdc.gov/violenceprevention/childabuseandneglect/fastfact.html. Child neglect refers to the failure to meet a child’s basic physical and emotional needs which includes housing, food, clothing, education, access to healthcare, and having feelings validated and appropriately responded to.2Centers for Disease Control and Prevention. Violence Prevention. Fast Facts: Preventing Child Abuse & Neglect. https://www.cdc.gov/violenceprevention/childabuseandneglect/fastfact.html. Child abuse and neglect (CAN), together also referred to as child maltreatment, affects children worldwide. The negative outcomes for abused children include but are not limited to poor educational achievement, mental health problems such as depression or anxiety, eating disorders, and age-inappropriate sexual behavior and/or knowledge.1Han H, Lees AB, Morse Z, Koziol-McLain J. Child abuse knowledge and attitudes among dental and oral health therapists in Aotearoa New Zealand: a cross-sectional study. BMC Health Serv Res 2022;22(1):1504. doi: 10.1186/s12913-022-08907-1. A majority of cases of CAN are not identified or reported, and intentional injury is often only discovered following death of the child.3Bailhache M, Leroy V, Pillet P, Salmi LR. Is early detection of abused children possible?: a systematic review of the diagnostic accuracy of the identification of abused children. BMC Pediatr 2013;13:202. doi: 10.1186/1471-2431-13-202.,4Massoni AC, Ferreira AM, Aragão AK et al. Aspectos orofaciais dos maus-tratos infantis e da negligência odontológica. [Orofacial aspects of childhood abuse and dental negligence]. Cien Saude Colet 2010;15(2):403-10. Portuguese. doi: 10.1590/S1413-81232010000200016. Only one third of children under the age of 5 years whose deaths were the result of child abuse in California for those born between 1999 and 2006 had previously been identified as victims of intentional physical abuse.3Bailhache M, Leroy V, Pillet P, Salmi LR. Is early detection of abused children possible?: a systematic review of the diagnostic accuracy of the identification of abused children. BMC Pediatr 2013;13:202. doi: 10.1186/1471-2431-13-202.,5Putnam-Hornstein E. Report of maltreatment as a risk factor for injury death: a prospective birth cohort study. Child Maltreat 2011;13(3):163-74. doi: 10.1177/1077559511411179.
Prevalence of CAN
According to the World Health Organization, estimates from 2016 showed that up to 1 billion children aged 2–17 years experienced CAN in the prior year.6World Health Organization. Violence against children. https://www.who.int/news-room/fact-sheets/detail/violence-against-children. Estimates on the number of children affected vary, with one report stating that up to 16% of children are physically abused in high-income areas, and up to 10% of girls and 5% of boys are sexually abused.7Gilbert R, Widom CS, Browne K et al. Burden and consequences of child maltreatment in high-income countries. Lancet 2009;373(9657):68-81. Based on data for 55,000 children born over a seventeen-year period in New Zealand, almost a quarter were estimated to be affected, and approximately 10% of children were confirmed to have suffered from CAN.8Rouland B, Vaithianathan R. Cumulative prevalence of maltreatment among New Zealand children, 1998–2015. Am J Public Health 2018;108(4):511-3. In the US, more than half a million children were reported to be victims of CAN in 2022.9U.S. Department of Health & Human Services. Children’s Bureau. Child Maltreatment. https://www.acf.hhs.gov/sites/default/files/documents/cb/cm2022.pdf.
Risk Factors for Child Abuse
Risk factors for child abuse include parental depression, substance abuse, inequalities and insecurities – notably housing and nutrition, and domestic violence in the household.1Han H, Lees AB, Morse Z, Koziol-McLain J. Child abuse knowledge and attitudes among dental and oral health therapists in Aotearoa New Zealand: a cross-sectional study. BMC Health Serv Res 2022;22(1):1504. doi: 10.1186/s12913-022-08907-1.,9U.S. Department of Health & Human Services. Children’s Bureau. Child Maltreatment. https://www.acf.hhs.gov/sites/default/files/documents/cb/cm2022.pdf. Other risks include having more than 2 siblings at home; lack of family support; and the child being unwanted or having a disability or other special needs.10Gonzalez D, Mirabal AB, McCall JD. Child Abuse and Neglect. National Library of Medicine. Statpearls. Update: July 4, 2023. https://www.ncbi.nlm.nih.gov/books/NBK459146/. ,11Garrocho-Rangel A, Márquez-Preciado R, Olguín-Vivar AI et al. Dentist attitudes and responsibilities concerning child sexual abuse. A review and a case report. J Clin Exp Dent 2015;7(3):e428-34. http://www.medicinaoral.com/odo/volumenes/v7i3/jcedv7i3p428.pdf.,12Anees W, Franco A, Manica S. Non-accidental head and neck injuries in children and adolescents. J Forensic Odontostomatol 2022;40(1):42-52.
The Role of Dental Professionals in Identifying and Reporting Child Abuse
Dental professionals throughout the United States, as well as all other healthcare professionals, are mandated to report suspected CAN to law enforcement agencies or social services (child protection services).13American Academy of Pediatrics Committee on Child Abuse and Neglect and the American Academy of Pediatric Dentistry Council on Clinical Affairs. Guideline on Oral and Dental Aspects of Child Abuse and Neglect. Pediatr Dent 2016;38(5):E73-76. The Child Abuse Prevention and Treatment Act (CAPTA) is focused on the prevention, identification, and treatment of CAN in the US.14English A. Mandatory Reporting of Human Trafficking: Potential Benefits and Risks of Harm. AMA J Ethics 201719(1):54-62. doi: 10.1001/journalofethics.2017.19.1.pfor1-1701. Under an amendment that became effective in 2017, severe forms of trafficking of minors and sex trafficking are also considered child abuse, and states have the option to consider individuals up to 24 years-of-age as victims.14English A. Mandatory Reporting of Human Trafficking: Potential Benefits and Risks of Harm. AMA J Ethics 201719(1):54-62. doi: 10.1001/journalofethics.2017.19.1.pfor1-1701. With respect to reluctance associated with fear of consequences for the individual reporting it in the United States, it should be noted that a 2019 CAPTA amendment, the ‘Victims of Child Abuse Act Reauthorization Act’, protects individuals making reports in good faith concerning CAN, as well as those providing information or help, from civil and criminal liability.
State definitions and laws vary, with differing levels of required evidence for ‘suspected’ CAN and differences in whether reporting should be to child protection services or law enforcement.9U.S. Department of Health & Human Services. Children’s Bureau. Child Maltreatment. https://www.acf.hhs.gov/sites/default/files/documents/cb/cm2022.pdf. ,15Hilotin-Lee LTA. Child Abuse Laws State-by-State. June 21, 2023. https://www.findlaw.com/family/child-abuse/child-abuse-laws-state-by-state.html.
Identifying Potential Child Abuse in the Dental Setting
Abused minors may attend a dental office for treatment due to abusive physical injuries or for unrelated care.10Gonzalez D, Mirabal AB, McCall JD. Child Abuse and Neglect. National Library of Medicine. Statpearls. Update: July 4, 2023. https://www.ncbi.nlm.nih.gov/books/NBK459146/. In either case, there is an opportunity to identify suspected child abuse, particularly when orofacial injuries are present. The head and neck region is frequently involved in child abuse, making a visit to the dental professional an important opportunity to identify and report suspected abuse.16Spiller LR. Orofacial manifestations of child maltreatment: A review. Dent Traumatol 2023 May 25. doi: 10.1111/edt.12852. ,17Cairns AM, Mok JYQ, Welbury RR. Injuries to the head, face, mouth and neck in physically abused children in a community setting. Int J Paediatr Dent 2005;15:310-8.,18Sarkar R, Ozanne-Smith J, Bassed R. Systematic Review of the Patterns of Orofacial Injuries in Physically Abused Children and Adolescents. Trauma Violence Abuse 2021;22(1):136-46. doi: 10.1177/1524838019827617.
Intra-oral injuries that can be indicative of physical abuse include trauma to the teeth and oral soft tissues, including the oral frena. Intra-oral and peri-oral injuries include bruising, abrasions, burns, lacerations, bite marks, scarring, lichenification, and fractured, avulsed, or displaced teeth.18Sarkar R, Ozanne-Smith J, Bassed R. Systematic Review of the Patterns of Orofacial Injuries in Physically Abused Children and Adolescents. Trauma Violence Abuse 2021;22(1):136-46. doi: 10.1177/1524838019827617.,19Fisher-Owens SA, Lukefahr JL, Tate AR, American Academy of Pediatric Dentistry, Council on Clinical Affairs, Council on Scientific Affairs, Ad Hoc Work Group on Child Abuse and Neglect, American Academy of Pediatrics, Section on Oral Health Committee on Child Abuse and Neglect. Oral and Dental Aspects of Child Abuse and Neglect. Pediatr Dent 2017;39(4):278-83. ,20Fisher-Owens SA, Lukefahr JL, Tate AR et al. Oral and Dental Aspects of Child Abuse and Neglect. Pediatrics 2017;140 (2):e20171487. https://doi.org/ 10.1542/peds.2017-1487.,21Duman C, Al-Batayneh OB, Ahmad S et al. Self-reported knowledge, attitudes, and practice of final-year dental students in relation to child abuse: A multi-centre study. Int J Paediatr Dent 2021;31:801-9. https:// doi.org/10.1111/ipd.12781.,22Pawils S, Lindeman T, Lemke R. Dental neglect and its perception in the dental practice. Int J Environ Res Public Health 2022;19(11):6408.,23Becker DB, Needleman HL, Kotelchuck M. Child abuse and dentistry: orofacial trauma and its recognition by dentists. J Am Dent Assoc 1978;97:24-8. https://doi.org/10.14219/ jada.archive.1978.0447. (Table 1) Lacerations and abrasions may be caused by blunt trauma or forced feeding, and the use of gags can manifest as bruising, scarring or lichenification at lip commisures.19Fisher-Owens SA, Lukefahr JL, Tate AR, American Academy of Pediatric Dentistry, Council on Clinical Affairs, Council on Scientific Affairs, Ad Hoc Work Group on Child Abuse and Neglect, American Academy of Pediatrics, Section on Oral Health Committee on Child Abuse and Neglect. Oral and Dental Aspects of Child Abuse and Neglect. Pediatr Dent 2017;39(4):278-83. Trauma to the oropharynx and current or previous fractures of the mandible and maxilla are also indicative of potential child abuse. In one survey, fractured teeth, oral bruising, lacerations, mandibular or maxillary fractures, and burns were present in 32%, 24%, 14%, 11% and 5% of child abuse cases, respectively.23Becker DB, Needleman HL, Kotelchuck M. Child abuse and dentistry: orofacial trauma and its recognition by dentists. J Am Dent Assoc 1978;97:24-8. https://doi.org/10.14219/ jada.archive.1978.0447. Bite marks may be present on the lips or facially. These are typically superficial, causing discoloration abrasions and bruising. Human bite marks can be differentiated from animal bites which typically involve deeper bites and torn soft tissue.21Duman C, Al-Batayneh OB, Ahmad S et al. Self-reported knowledge, attitudes, and practice of final-year dental students in relation to child abuse: A multi-centre study. Int J Paediatr Dent 2021;31:801-9. https:// doi.org/10.1111/ipd.12781. Of note, the identification of perpetrators of crimes through bite mark identification is controversial.19Fisher-Owens SA, Lukefahr JL, Tate AR, American Academy of Pediatric Dentistry, Council on Clinical Affairs, Council on Scientific Affairs, Ad Hoc Work Group on Child Abuse and Neglect, American Academy of Pediatrics, Section on Oral Health Committee on Child Abuse and Neglect. Oral and Dental Aspects of Child Abuse and Neglect. Pediatr Dent 2017;39(4):278-83.
Table 1. Intraoral and peri-oral manifestations of potential abuse
| Physical abuse | Sexual abuse |
|---|---|
| Bruising | Petechiae at the junction of the hard and soft palate |
| Abrasions | Erythema |
| Burns | Ulcers |
| Lacerations | Torn oral frena |
| Scarring and lichenification | Sexually-transmitted infections |
| Bite marks | Papular-vescicobollous lesions and pseudomembranous areas (gonorrhea) |
| Fractured/avulsed/displaced teeth | Labial papule (syphilis) |
| Maxillary/mandibular fractures | Warts (HPV) |
Oral sexual abuse is reported to be a frequent form of child abuse; however, visible manifestations are not common.13American Academy of Pediatrics Committee on Child Abuse and Neglect and the American Academy of Pediatric Dentistry Council on Clinical Affairs. Guideline on Oral and Dental Aspects of Child Abuse and Neglect. Pediatr Dent 2016;38(5):E73-76. Petechiae present at the junction of the hard and soft palate may be present in cases where forced oral sex occurred.19Fisher-Owens SA, Lukefahr JL, Tate AR, American Academy of Pediatric Dentistry, Council on Clinical Affairs, Council on Scientific Affairs, Ad Hoc Work Group on Child Abuse and Neglect, American Academy of Pediatrics, Section on Oral Health Committee on Child Abuse and Neglect. Oral and Dental Aspects of Child Abuse and Neglect. Pediatr Dent 2017;39(4):278-83. Other indications of potential sexual abuse include erythema, ulcers, torn frena and sexually-transmitted infections (STDs). Oral and peri-oral manifestations of STDs, while uncommon, include ulcers, redness and papular-vesicobollous lesions and pseudomembranous areas in cases of gonorrhea, and syphilis may present with a labial papule.24Costacurta M, Benavoli D, Arcudi G, Docimo R. Oral and dental signs of child abuse and neglect. Oral & Implantol 2015;8:68-73. Infection with HPV may result in oral and peri-oral warts.13American Academy of Pediatrics Committee on Child Abuse and Neglect and the American Academy of Pediatric Dentistry Council on Clinical Affairs. Guideline on Oral and Dental Aspects of Child Abuse and Neglect. Pediatr Dent 2016;38(5):E73-76. (Table 1)
Dental neglect is defined by the American Academy of Pediatric Dentistry (AAPD) as the “willful failure of parent or guardian, despite adequate access to care, to seek and follow through with treatment necessary to ensure a level of oral health essential for adequate function and freedom from pain and infection.”19Fisher-Owens SA, Lukefahr JL, Tate AR, American Academy of Pediatric Dentistry, Council on Clinical Affairs, Council on Scientific Affairs, Ad Hoc Work Group on Child Abuse and Neglect, American Academy of Pediatrics, Section on Oral Health Committee on Child Abuse and Neglect. Oral and Dental Aspects of Child Abuse and Neglect. Pediatr Dent 2017;39(4):278-83. Dental neglect can manifest as rampant and untreated dental caries, abscesses, and untreated dental trauma.25Spiller L, Lukefahr J, Kellogg N. Dental Neglect. J Child Adolesc Trauma 2019;13(3):299-303. doi: 10.1007/s40653-019-0247-y. It is important to note that there can be circumstances under which untreated dental caries is present for reasons other than neglect (including lack of access to care).
Red flags for suspected child abuse
There are specific red flags that further support suspicion of child abuse.10Gonzalez D, Mirabal AB, McCall JD. Child Abuse and Neglect. National Library of Medicine. Statpearls. Update: July 4, 2023. https://www.ncbi.nlm.nih.gov/books/NBK459146/. ,12Anees W, Franco A, Manica S. Non-accidental head and neck injuries in children and adolescents. J Forensic Odontostomatol 2022;40(1):42-52. These include injuries that are inconsistent with the cause stated by the parent/caregiver, injuries that are incongruent with the age of the child, and an inadequate/incomplete history for the injury. Furthermore, the location an injury can suggest abuse/non-abuse. For example, bruising of the head and face is most common in abused children while, conversely, bruising of the front of the lower legs (shins and knees) is most common in non-abused children.10Gonzalez D, Mirabal AB, McCall JD. Child Abuse and Neglect. National Library of Medicine. Statpearls. Update: July 4, 2023. https://www.ncbi.nlm.nih.gov/books/NBK459146/. Head and neck injuries were present in 59% of more than 300 cases of child abuse in one research study.17Cairns AM, Mok JYQ, Welbury RR. Injuries to the head, face, mouth and neck in physically abused children in a community setting. Int J Paediatr Dent 2005;15:310-8. This finding is corroborated by other research where head and neck injuries were present in approximately 50 to 70% of cases of child abuse.12Anees W, Franco A, Manica S. Non-accidental head and neck injuries in children and adolescents. J Forensic Odontostomatol 2022;40(1):42-52.,23Becker DB, Needleman HL, Kotelchuck M. Child abuse and dentistry: orofacial trauma and its recognition by dentists. J Am Dent Assoc 1978;97:24-8. https://doi.org/10.14219/ jada.archive.1978.0447.,26Jessee SA. Orofacial manifestations of child abuse and neglect. Am Fam Physician 1995;52(6):1829-34. ,27Yu YR, DeMello AS, Greeley CS et al. Injury patterns of child abuse: Experience of two Level 1 pediatric trauma centers. J Pediatric Surg 2018;53(5):1028-32.,28Sheets LK, Leach ME, Koszewski IJ et al. Sentinel injuries in infants evaluated for child physical abuse. Pediatrics 2013;131:701-7. doi:10.1542/peds.2012-2780.
Increased suspicion should be present if the parent/caregiver shows a lack of concern, the visit for care is delayed, or if the child seem fearful, withdrawn or relates things regarding the injury/event differently.
Barriers to Child Abuse Reporting by Dental Professionals
Figure 1. Factors influencing the percentage of dental professionals in New Zealand in not reporting suspected child abuse1Han H, Lees AB, Morse Z, Koziol-McLain J. Child abuse knowledge and attitudes among dental and oral health therapists in Aotearoa New Zealand: a cross-sectional study. BMC Health Serv Res 2022;22(1):1504. doi: 10.1186/s12913-022-08907-1.
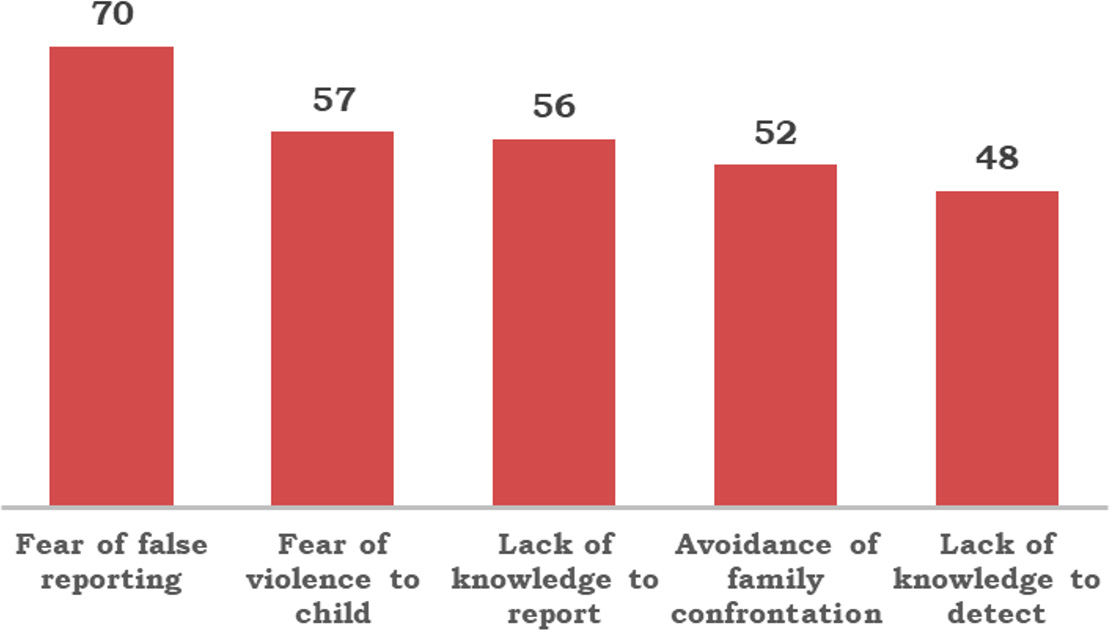
Figure 2. Factors influencing the percentage of dental professionals in Scotland in not reporting suspected child abuse29Harris CM, Welbury R, Cairns AM. The Scottish dental practitioner’s role in managing child abuse and neglect. Br Dent J 2013;214:E24. https://doi.org/10.1038/ sj.bdj.2013.435.
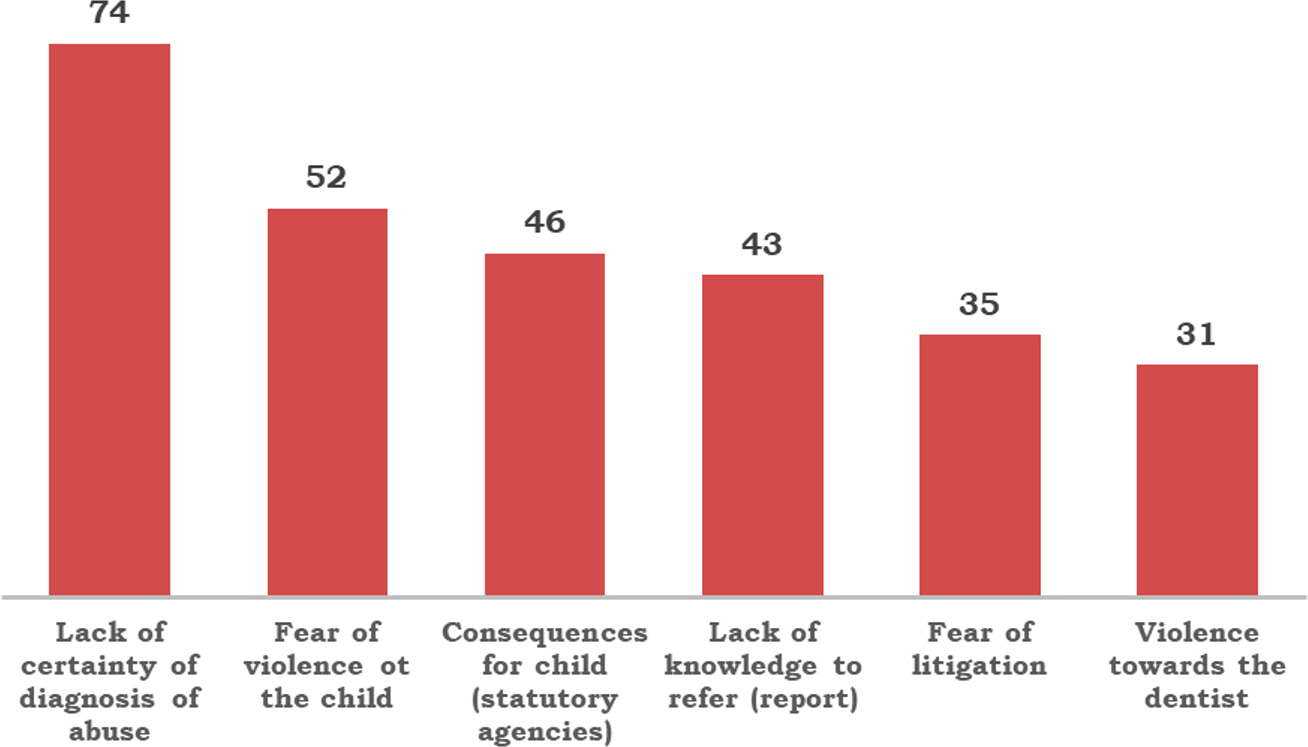
The outcomes of several surveys show that there are significant barriers to reporting child abuse.1Han H, Lees AB, Morse Z, Koziol-McLain J. Child abuse knowledge and attitudes among dental and oral health therapists in Aotearoa New Zealand: a cross-sectional study. BMC Health Serv Res 2022;22(1):1504. doi: 10.1186/s12913-022-08907-1. Barriers noted recently in a New Zealand survey of dentists and oral health therapists included fear of false reporting by 70% of respondents, while the other main concerns included fear of the outcome of reporting – specifically that physical abuse of the child would increase, lack of knowledge to report potential abuse, avoidance of family confrontation, and lack of knowledge to detect potential child abuse were cited by 57%,56%, 52% and 48%, respectively.1Han H, Lees AB, Morse Z, Koziol-McLain J. Child abuse knowledge and attitudes among dental and oral health therapists in Aotearoa New Zealand: a cross-sectional study. BMC Health Serv Res 2022;22(1):1504. doi: 10.1186/s12913-022-08907-1. (Figure 1) In a survey conducted in Scotland in 2010, failure to report suspected CAN was found to be most influenced by lack of certainty of the diagnosis (fear of false reporting) and cited by 74% of respondents. Fear of violence to the child, consequences for the child from statutory agencies, lack of knowledge of the referral process, fear of litigation and of violence against the dentist were reported by 52%, 46%, 43%, 35% and 31% of respondents, respectively. Furthermore, while 37% of respondents had seen patients where they suspected CAN, suspected cases were referred by only 11% of respondents.29Harris CM, Welbury R, Cairns AM. The Scottish dental practitioner’s role in managing child abuse and neglect. Br Dent J 2013;214:E24. https://doi.org/10.1038/ sj.bdj.2013.435. (Figure 2) Similar barriers have been noted in other studies.12Anees W, Franco A, Manica S. Non-accidental head and neck injuries in children and adolescents. J Forensic Odontostomatol 2022;40(1):42-52.,29Harris CM, Welbury R, Cairns AM. The Scottish dental practitioner’s role in managing child abuse and neglect. Br Dent J 2013;214:E24. https://doi.org/10.1038/ sj.bdj.2013.435.,30Bjørknes R, Iversen AC, Nordrehaug Åstrøm A, Vaksdal Brattabø I. Why are they reluctant to report? A study of the barriers to reporting to child welfare services among public dental healthcare personnel. Health Soc Care Community 2019;27(4):871-9. doi: 10.1111/hsc.12703.,31Nunes LS, Silva-Oliveira F, Mattos FF et al. Prevalence of recognition and reporting of child physical abuse by dental surgeons and associated factors. Cien Saude Colet 2021;26:5013-22. https://doi.org/10.1590/1413-812320212611.3.02442020. ,32Mascarenhas A, Deshmukh A, Scott T. New England, USA dental professionals' attitudes and behaviours regarding domestic violence. Br Dent J 2009;206:E5. https://doi.org/10.1038/sj.bdj.2009.7.,33Clarke L, Chana P, Nazzal H et al. Experience of and barriers to reporting child safeguarding concerns among general dental practitioners across Greater Manchester. Br Dent J 2019;227:387-91. https://doi.org/10.1038/s41415-019-0663-2.
Dissonance between self-perceived knowledge and the results of testing knowledge on child abuse may also be an issue. In a recent survey with 61 respondents across 10 countries, 83% stated they had sufficient knowledge of injuries related to child abuse and neglect and 61% that they knew how to manage suspected abuse.12Anees W, Franco A, Manica S. Non-accidental head and neck injuries in children and adolescents. J Forensic Odontostomatol 2022;40(1):42-52. However, few participants were able to identify signs of child abuse when given scenarios or inconsistencies in information provided on how injuries occurred. In one study of final-year dental students in 11 dental schools in 10 countries, it was also found that dental students’ knowledge varied by country and that they had difficulty identifying CAN.21Duman C, Al-Batayneh OB, Ahmad S et al. Self-reported knowledge, attitudes, and practice of final-year dental students in relation to child abuse: A multi-centre study. Int J Paediatr Dent 2021;31:801-9. https:// doi.org/10.1111/ipd.12781. Eighty-six percent of the final-year students indicated the desire for additional training.
Training
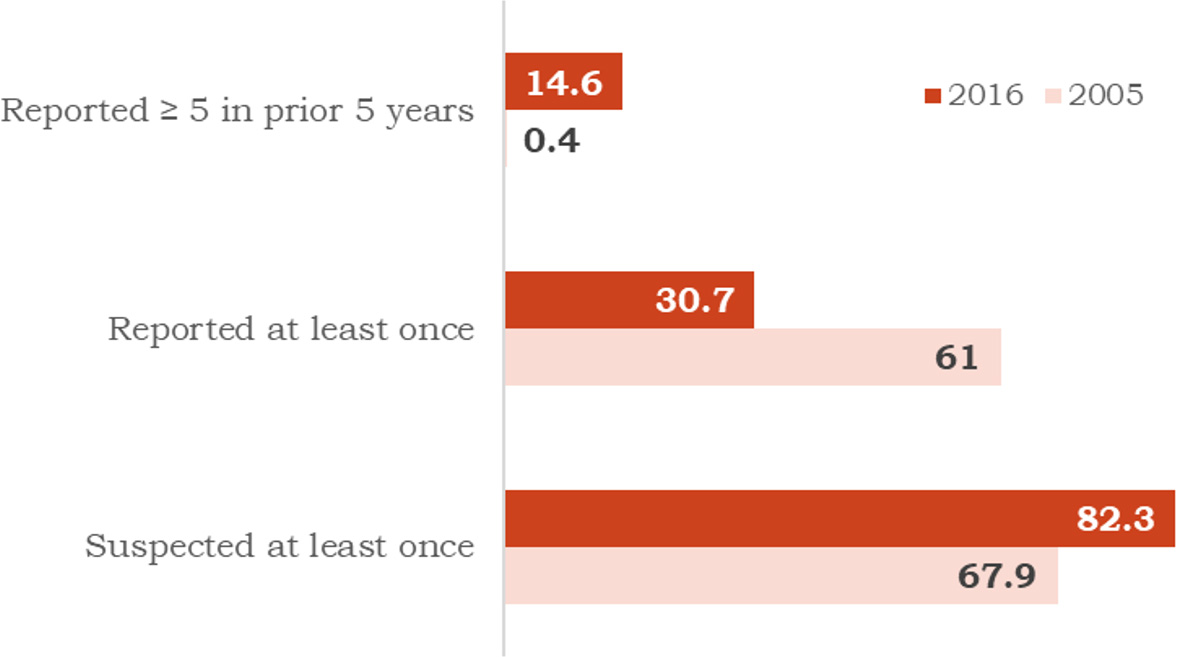
Figure 3. Changes in the percentage of pediatric dentists suspecting and reporting CAN over time34Harris JC, Baker SR, Elcock C. Paediatric dentists' role in child protection practice: Progress over time? Int J Paediatr Dent 2022;32:714-23. doi:10.1111/ipd.12950.
It is generally acknowledged by respondents in surveys that training – both initial training and additional training – is required and would increase the ability of dental professionals to identify and report potential CAN. Studies comparing the propensity of dental professionals to report suspected CAN also indicate changes over time with increased training and information on CAN. In one study, the responses of pediatric dentists were compared for surveys conducted in 2005 and 2016.34Harris JC, Baker SR, Elcock C. Paediatric dentists' role in child protection practice: Progress over time? Int J Paediatr Dent 2022;32:714-23. doi:10.1111/ipd.12950. It was found that the percentage of pediatric dentists identifying and reporting suspected CAN increased with training. By 2016, almost all respondents had received post-graduate child protection training. In comparing 2016 with 2005, 82.3% and 67.9% respectively had suspected CAN at least once, and 61% and 30.7%, respectively, had reported CAN at least once. Additionally, the number reporting CAN at least five times in the prior five years increased to 14.6% by 2016 (from 0.4% in 2005). (Figure 3) Other studies supports these findings, where training improved results between timepoints.29Harris CM, Welbury R, Cairns AM. The Scottish dental practitioner’s role in managing child abuse and neglect. Br Dent J 2013;214:E24. https://doi.org/10.1038/ sj.bdj.2013.435. State Dental Boards can mandate training in CAN for licensing and license renewal.
Conclusions
CAN is a tragic occurrence, with significant and far-reaching consequences for victims. In the United States, all other healthcare professionals are mandated to report suspected CAN. In addition, research has shown that additional training in identifying signs of suspected cases leads to increases in reporting and is recommended. In conclusion, dental professionals play a key role in identifying manifestations of CAN in the orofacial region and reporting this in accordance with Federal and state requirements.
References
- 1.Han H, Lees AB, Morse Z, Koziol-McLain J. Child abuse knowledge and attitudes among dental and oral health therapists in Aotearoa New Zealand: a cross-sectional study. BMC Health Serv Res 2022;22(1):1504. doi: 10.1186/s12913-022-08907-1.
- 2.Centers for Disease Control and Prevention. Violence Prevention. Fast Facts: Preventing Child Abuse & Neglect. https://www.cdc.gov/violenceprevention/childabuseandneglect/fastfact.html.
- 3.Bailhache M, Leroy V, Pillet P, Salmi LR. Is early detection of abused children possible?: a systematic review of the diagnostic accuracy of the identification of abused children. BMC Pediatr 2013;13:202. doi: 10.1186/1471-2431-13-202.
- 4.Massoni AC, Ferreira AM, Aragão AK et al. Aspectos orofaciais dos maus-tratos infantis e da negligência odontológica. [Orofacial aspects of childhood abuse and dental negligence]. Cien Saude Colet 2010;15(2):403-10. Portuguese. doi: 10.1590/S1413-81232010000200016.
- 5.Putnam-Hornstein E. Report of maltreatment as a risk factor for injury death: a prospective birth cohort study. Child Maltreat 2011;13(3):163-74. doi: 10.1177/1077559511411179.
- 6.World Health Organization. Violence against children. https://www.who.int/news-room/fact-sheets/detail/violence-against-children.
- 7.Gilbert R, Widom CS, Browne K et al. Burden and consequences of child maltreatment in high-income countries. Lancet 2009;373(9657):68-81.
- 8.Rouland B, Vaithianathan R. Cumulative prevalence of maltreatment among New Zealand children, 1998–2015. Am J Public Health 2018;108(4):511-3.
- 9.U.S. Department of Health & Human Services. Children’s Bureau. Child Maltreatment. https://www.acf.hhs.gov/sites/default/files/documents/cb/cm2022.pdf.
- 10.Gonzalez D, Mirabal AB, McCall JD. Child Abuse and Neglect. National Library of Medicine. Statpearls. Update: July 4, 2023. https://www.ncbi.nlm.nih.gov/books/NBK459146/.
- 11.Garrocho-Rangel A, Márquez-Preciado R, Olguín-Vivar AI et al. Dentist attitudes and responsibilities concerning child sexual abuse. A review and a case report. J Clin Exp Dent 2015;7(3):e428-34. http://www.medicinaoral.com/odo/volumenes/v7i3/jcedv7i3p428.pdf.
- 12.Anees W, Franco A, Manica S. Non-accidental head and neck injuries in children and adolescents. J Forensic Odontostomatol 2022;40(1):42-52.
- 13.American Academy of Pediatrics Committee on Child Abuse and Neglect and the American Academy of Pediatric Dentistry Council on Clinical Affairs. Guideline on Oral and Dental Aspects of Child Abuse and Neglect. Pediatr Dent 2016;38(5):E73-76.
- 14.English A. Mandatory Reporting of Human Trafficking: Potential Benefits and Risks of Harm. AMA J Ethics 201719(1):54-62. doi: 10.1001/journalofethics.2017.19.1.pfor1-1701.
- 15.Hilotin-Lee LTA. Child Abuse Laws State-by-State. June 21, 2023. https://www.findlaw.com/family/child-abuse/child-abuse-laws-state-by-state.html.
- 16.Spiller LR. Orofacial manifestations of child maltreatment: A review. Dent Traumatol 2023 May 25. doi: 10.1111/edt.12852.
- 17.Cairns AM, Mok JYQ, Welbury RR. Injuries to the head, face, mouth and neck in physically abused children in a community setting. Int J Paediatr Dent 2005;15:310-8.
- 18.Sarkar R, Ozanne-Smith J, Bassed R. Systematic Review of the Patterns of Orofacial Injuries in Physically Abused Children and Adolescents. Trauma Violence Abuse 2021;22(1):136-46. doi: 10.1177/1524838019827617.
- 19.Fisher-Owens SA, Lukefahr JL, Tate AR, American Academy of Pediatric Dentistry, Council on Clinical Affairs, Council on Scientific Affairs, Ad Hoc Work Group on Child Abuse and Neglect, American Academy of Pediatrics, Section on Oral Health Committee on Child Abuse and Neglect. Oral and Dental Aspects of Child Abuse and Neglect. Pediatr Dent 2017;39(4):278-83.
- 20.Fisher-Owens SA, Lukefahr JL, Tate AR et al. Oral and Dental Aspects of Child Abuse and Neglect. Pediatrics 2017;140 (2):e20171487. https://doi.org/ 10.1542/peds.2017-1487.
- 21.Duman C, Al-Batayneh OB, Ahmad S et al. Self-reported knowledge, attitudes, and practice of final-year dental students in relation to child abuse: A multi-centre study. Int J Paediatr Dent 2021;31:801-9. https:// doi.org/10.1111/ipd.12781.
- 22.Pawils S, Lindeman T, Lemke R. Dental neglect and its perception in the dental practice. Int J Environ Res Public Health 2022;19(11):6408.
- 23.Becker DB, Needleman HL, Kotelchuck M. Child abuse and dentistry: orofacial trauma and its recognition by dentists. J Am Dent Assoc 1978;97:24-8. https://doi.org/10.14219/ jada.archive.1978.0447.
- 24.Costacurta M, Benavoli D, Arcudi G, Docimo R. Oral and dental signs of child abuse and neglect. Oral & Implantol 2015;8:68-73.
- 25.Spiller L, Lukefahr J, Kellogg N. Dental Neglect. J Child Adolesc Trauma 2019;13(3):299-303. doi: 10.1007/s40653-019-0247-y.
- 26.Jessee SA. Orofacial manifestations of child abuse and neglect. Am Fam Physician 1995;52(6):1829-34.
- 27.Yu YR, DeMello AS, Greeley CS et al. Injury patterns of child abuse: Experience of two Level 1 pediatric trauma centers. J Pediatric Surg 2018;53(5):1028-32.
- 28.Sheets LK, Leach ME, Koszewski IJ et al. Sentinel injuries in infants evaluated for child physical abuse. Pediatrics 2013;131:701-7. doi:10.1542/peds.2012-2780.
- 29.Harris CM, Welbury R, Cairns AM. The Scottish dental practitioner’s role in managing child abuse and neglect. Br Dent J 2013;214:E24. https://doi.org/10.1038/ sj.bdj.2013.435.
- 30.Bjørknes R, Iversen AC, Nordrehaug Åstrøm A, Vaksdal Brattabø I. Why are they reluctant to report? A study of the barriers to reporting to child welfare services among public dental healthcare personnel. Health Soc Care Community 2019;27(4):871-9. doi: 10.1111/hsc.12703.
- 31.Nunes LS, Silva-Oliveira F, Mattos FF et al. Prevalence of recognition and reporting of child physical abuse by dental surgeons and associated factors. Cien Saude Colet 2021;26:5013-22. https://doi.org/10.1590/1413-812320212611.3.02442020.
- 32.Mascarenhas A, Deshmukh A, Scott T. New England, USA dental professionals' attitudes and behaviours regarding domestic violence. Br Dent J 2009;206:E5. https://doi.org/10.1038/sj.bdj.2009.7.
- 33.Clarke L, Chana P, Nazzal H et al. Experience of and barriers to reporting child safeguarding concerns among general dental practitioners across Greater Manchester. Br Dent J 2019;227:387-91. https://doi.org/10.1038/s41415-019-0663-2.
- 34.Harris JC, Baker SR, Elcock C. Paediatric dentists' role in child protection practice: Progress over time? Int J Paediatr Dent 2022;32:714-23. doi:10.1111/ipd.12950.