

Eating Disorders and Patient Management Strategies
Eating disorders (ED), more recently denoted as Feeding and Eating Disorders by the American Psychiatric Association (APA) and World Health Organization, are prevalent conditions worldwide.1American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, Va: American Psychiatric Association; 2013:338-350.,2World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 11th Revision (ICD‐11). Geneva:World Health Organization; 2019.,3Galmiche M, Déchelotte P, Lambert G, Tavolacci MP. Prevalence of eating disorders over the 2000-2018 period: a systematic literature review. Am J Clin Nutr 2019;109(5):1402-1413. doi: 10.1093/ajcn/nqy342. Based on a systematic review, the prevalence of ED increased to 7.8% between 2013 and 2017, from 3.5% for 2000 to 2006.3Galmiche M, Déchelotte P, Lambert G, Tavolacci MP. Prevalence of eating disorders over the 2000-2018 period: a systematic literature review. Am J Clin Nutr 2019;109(5):1402-1413. doi: 10.1093/ajcn/nqy342. In the US, it is estimated that 28.8 million individuals will suffer from ED during their lifetime.4Deloitte Access Economics. The Social and Economic Cost of Eating Disorders in the United States of America: A Report for the Strategic Training Initiative for the Prevention of Eating Disorders and the Academy for Eating Disorders. June 2020. https://www.hsph.harvard.edu/striped/report-economic-costs-of-eating-disorders/. In addition, these disorders are more prevalent in females, typically first appearing in younger individuals.5National Institute of Mental Health. Eating Disorders. https://www.nimh.nih.gov/health/topics/eating-disorders. ED includes anorexia nervosa (AN), bulimia nervosa (BN), binge-eating disorder, and avoidant/restrictive food intake disorder.5National Institute of Mental Health. Eating Disorders. https://www.nimh.nih.gov/health/topics/eating-disorders.,6Hay P. Current approach to eating disorders: a clinical update. Intern Med J 2020;50(1):24-29. doi:10.1111/imj.14691. In this article, we will discuss AN and BN, their impact on oral and systemic health, and the role of dental professionals.
Figure 1. Distorted view of body image

Characteristics of AN and BN
Individuals with AN range from being underweight with a body mass index (BMI) of <18 kg/m2 to extremely thin.1American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, Va: American Psychiatric Association; 2013:338-350. This syndrome includes individuals who severely reduce their caloric intake and individuals engaging in both caloric reduction and binging-purging. Affected individuals may also exercise excessively in order to control weight and may/may not have an intense fear of becoming fat.1American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, Va: American Psychiatric Association; 2013:338-350.,7Lo Russo L, Campisi G, Di Fede O, et al. Oral manifestations of eating disorders: a critical review. Oral Dis 2008;14(6):479-484. Individuals with BN are of normal weight or overweight and indulge in uncontrolled binge-eating followed by purging achieved by vomiting, use of strong laxatives, exercise, enemas or diuretics.5National Institute of Mental Health. Eating Disorders. https://www.nimh.nih.gov/health/topics/eating-disorders. In accordance with the APA diagnostic criteria for BN, binge-eating and purging must occur at least once a week for a minimum of 3 months.1American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, Va: American Psychiatric Association; 2013:338-350. There is overlap in the behaviors of individuals with AN and BN. More than half of individuals with AN also engage in bulimic behavior with self-induced vomiting (SIV), and atypical BN with binge-eating and severe caloric restriction and/or aggressive exercise regimens also exists.6Hay P. Current approach to eating disorders: a clinical update. Intern Med J 2020;50(1):24-29. doi:10.1111/imj.14691.,8Milosevic A. Eating disorders and the dentist. Br Dent J 1999;186:109-113. https://doi.org/10.1038/sj.bdj.4800036. In both AN and BN, the patient has a distorted view of their body image. (Figure 1)
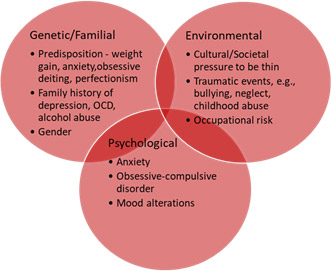
Figure 2. Risk factors for AN and BN
Risk Factors
Risk factors for ED include genetic, environmental and psychological factors.9Bulik CM, Blake L, Austin J. Genetics of Eating Disorders: What the Clinician Needs to Know. Psychiatr Clin North Am 2019;42(1):59-73. doi: 10.1016/j.psc.2018.10.007.,10Gaudio S, Quattrocchi CC. Neural basis of a multidimensional model of body image distortion in anorexia nervosa. Neurosci Biobehav Rev 2012;36(8):1839-1847. doi: 10.1016/j.neubiorev.2012.05.003. Genetic factors include a neural predisposition, and predispositions for perfectionism, anxiety, weight gain and associated obsessive dieting.7Lo Russo L, Campisi G, Di Fede O, et al. Oral manifestations of eating disorders: a critical review. Oral Dis 2008;14(6):479-484.,10Gaudio S, Quattrocchi CC. Neural basis of a multidimensional model of body image distortion in anorexia nervosa. Neurosci Biobehav Rev 2012;36(8):1839-1847. doi: 10.1016/j.neubiorev.2012.05.003.,11Lulé D, Schulze UME, Bauer K, et al. Anorexia nervosa and its relation to depression, anxiety, alexithymia and emotional processing deficits. Eat Weight Disord 2014;19:209-216. Studies in identical twins and more recently genome-wide research have confirmed the role of genetics.8Milosevic A. Eating disorders and the dentist. Br Dent J 1999;186:109-113. https://doi.org/10.1038/sj.bdj.4800036.,9Bulik CM, Blake L, Austin J. Genetics of Eating Disorders: What the Clinician Needs to Know. Psychiatr Clin North Am 2019;42(1):59-73. doi: 10.1016/j.psc.2018.10.007. BN is considered to have a heritability of 0.60.9Bulik CM, Blake L, Austin J. Genetics of Eating Disorders: What the Clinician Needs to Know. Psychiatr Clin North Am 2019;42(1):59-73. doi: 10.1016/j.psc.2018.10.007. Gender is also a risk factor, with an 11-fold risk of AN for females if they have relatives with this condition. Environmental factors include cultural / societal pressures to be thin, especially for adolescent and young adult females.8Milosevic A. Eating disorders and the dentist. Br Dent J 1999;186:109-113. https://doi.org/10.1038/sj.bdj.4800036.,12Westmoreland P, Krantz MJ, Mehler PS. Medical Complications of Anorexia Nervosa and Bulimia. Am J Med 2016;129(1):30-37. doi: 10.1016/j.amjmed.2015.06.031. Familial factors include a history of depression, obsessive-compulsive disorder (OCD) and alcohol abuse.9Bulik CM, Blake L, Austin J. Genetics of Eating Disorders: What the Clinician Needs to Know. Psychiatr Clin North Am 2019;42(1):59-73. doi: 10.1016/j.psc.2018.10.007. Traumatic events such as childhood abuse, neglect and bullying are also risk factors.8Milosevic A. Eating disorders and the dentist. Br Dent J 1999;186:109-113. https://doi.org/10.1038/sj.bdj.4800036. In addition, weight control creates an occupational risk factor for models, ballerinas, ice skaters, gymnasts and other athletes where lean body mass is preferred.13Mancine RP, Gusfa DW, Moshrefi A, et al. Prevalence of disordered eating in athletes categorized by emphasis on leanness and activity type – a systematic review. J Eat Disord 2020;8:47. https://doi.org/10.1186/s40337-020-00323-2. (Figure 2)
Systemic Health Impact
Severe morbidity and mortality can occur with AN and BN. At extremely low weights, patients suffer from cardiovascular disease, metabolic and endocrine dysfunction. Among individuals with severe AN and malnutrition, BMI may be very low and, at a lifetime average of 10.5kg/m2, 45% of individuals will die prematurely.14Gaudiani JL, Braverman JM, Mascolo M, Mehler PS. Ophthalmic changes in severe anorexia nervosa: a case series. Int J Eat Disord 2012;45(5):719-721. doi: 10.1002/eat.20970. Individuals with BN also experience higher mortality rates than the general population.15Crow SJ, Peterson CB, Swanson SA, et al. Increased mortality in bulimia nervosa and other eating disorders. Am J Psychiatry 2009;166:1342-1346. Furthermore, attempted suicide is reported in approximately 1 in 4 individuals with ED. AN is associated with gastrointestinal disorders including dysphagia, slowed gastric emptying, nausea, bloating and potential for gastric perforation.16Lin JA, Woods ER, Bern EM. Common and Emergent Oral and Gastrointestinal Manifestations of Eating Disorders. Gastroenterol Hepatol (NY) 2021;17(4):157-167. Other conditions include fatty liver, cardiovascular disease, renal disease, anemia, leukopenia, thrombocytopenia, a suppressed immune system, amenorrhea with subsequent osteopenia/osteoporosis, thyroid abnormalities, risk for infertility, multi-organ failure and brain damage.5National Institute of Mental Health. Eating Disorders. https://www.nimh.nih.gov/health/topics/eating-disorders.,7Lo Russo L, Campisi G, Di Fede O, et al. Oral manifestations of eating disorders: a critical review. Oral Dis 2008;14(6):479-484.,12Westmoreland P, Krantz MJ, Mehler PS. Medical Complications of Anorexia Nervosa and Bulimia. Am J Med 2016;129(1):30-37. doi: 10.1016/j.amjmed.2015.06.031. In addition, individuals experience thinning of hair while displaying fine pigmented hair on their body and face known as lanugo, severe acne, brittle nails, dry and yellowish skin, or may have cyanotic bluish skin. Hypertension, ulcers, diabetes, constipation, anxiety, depression, and other physical and mental illness occur in patients with AN or BN, and quality-of-life is severely impacted.16Lin JA, Woods ER, Bern EM. Common and Emergent Oral and Gastrointestinal Manifestations of Eating Disorders. Gastroenterol Hepatol (NY) 2021;17(4):157-167.,17Ágh T, Kovács G, Supina D, et al. A systematic review of the health-related quality of life and economic burdens of anorexia nervosa, bulimia nervosa, and binge eating disorder. Eat Weight Disord 2016;21(3):353-364. doi:10.1007/s40519-016-0264-x.18. (Table 1)
| Table 1. Systemic health impact of ANa |
|---|
| Cardiovascular disease |
| Metabolic and endocrine dysfunction |
| Gastrointestinal disorders |
| Fatty liver |
| Renal disease |
| Blood disorders |
| Suppressed immune system |
| Amenorrhea and risk for infertility |
| Osteopenia/osteoporosis |
| Thyroid abnormalities |
| Brain damage |
| Multi-organ failure |
| Thinning hair and lanugo |
| Skin alterations |
| Diabetes |
| Mental disorders, including suicidal thoughts and suicide |
a Effects of bulimic behavior are contained in Table 2
Individuals with BN or bulimic behavior have severe electrolyte disturbances. SIV is achieved by placing fingers or an object down the throat or by using ipecac syrup, a cumulative toxin causing cardiovascular complications.18Mickley D, Greenfeld D, Quinlan DM, et al. Abnormal liver enzymes in outpatients with eating disorders. Int J Eat Disord 1996;20(3):325-329. Repeated vomiting results in ongoing acid reflux, dysphagia, dyspepsia (indigestion), laryngeal damage, hoarseness, hematemesis, potential for esophageal rupture/malignancy, pancreatitis, metabolic alkalosis and hypokalemia which in severe cases cause cardiac arrythmias, epistaxis (bleeding from the nose), subconjunctival hemorrhages and sialadenitis.12Westmoreland P, Krantz MJ, Mehler PS. Medical Complications of Anorexia Nervosa and Bulimia. Am J Med 2016;129(1):30-37. doi: 10.1016/j.amjmed.2015.06.031.,15Crow SJ, Peterson CB, Swanson SA, et al. Increased mortality in bulimia nervosa and other eating disorders. Am J Psychiatry 2009;166:1342-1346.,17Ágh T, Kovács G, Supina D, et al. A systematic review of the health-related quality of life and economic burdens of anorexia nervosa, bulimia nervosa, and binge eating disorder. Eat Weight Disord 2016;21(3):353-364. doi:10.1007/s40519-016-0264-x.18. (Table 2) Extended use of laxatives causes lower intestinal tract complications. In addition to physical manifestations, individuals with AN and BN are at risk for substance abuse, promiscuity, and committing theft.1American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, Va: American Psychiatric Association; 2013:338-350.
| Table 2. Effects of repeated vomiting |
|---|
| Severe electrolyte disturbances |
| Acid reflux |
| Dysphagia and dyspepsia |
| Laryngeal damage and hoarseness |
| Potential for esophageal rupture/malignancy |
| Hematemesis |
| Pancreatitis |
| Metabolic alkalosis and hypokalemia |
| Cardiac arrythmias |
| Epistaxis |
| Subconjunctival hemorrhages |
| Bilateral enlargement of parotid glands |
Oral Manifestations
Oral manifestations involving peri-oral and intra-oral tissues are present in patients with AN and BN.7Lo Russo L, Campisi G, Di Fede O, et al. Oral manifestations of eating disorders: a critical review. Oral Dis 2008;14(6):479-484.,19Monda M, Costacurta M, Maffei L, Docimo R. Oral manifestations of eating disorders in adolescent patients. A review. Eur J Paediatr Dent 2021;22(2):155-158. doi: 10.23804/ejpd.2021.22.02.13.,20De Bate R, Tedesco LA, Kerschbaum WE. Knowledge of Oral and Physical Manifestations of Anorexia and Bulimia Nervosa Among Dentists and Dental Hygienists. J Dent Ed 2005;69(3):346-354.,21Lourenço M, Azevedo Á, Brandão I, Gomes PS. Orofacial manifestations in outpatients with anorexia nervosa and bulimia nervosa focusing on the vomiting behavior. Clin Oral Investig 2018;22(5):1915-1922. doi: 10.1007/s00784-017-2284-y.,22National Eating Disorders Association. Dental complications of eating disorders. nationaleatingdisorders.org/dental-complications-eating-disorders.,23Panico R, Piemonte E, Lazos J, et al. Oral mucosal lesions in anorexia nervosa, bulimia nervosa and EDNOS. J Psychiatr Res 2018;96:178-182.,24Garrido-Martínez P, Domínguez-Gordillo A, Cerero-Lapiedra R, et al. Oral and dental health status in patients with eating disorders in Madrid, Spain. Med Oral Patol Oral Cir Bucal 2019;24(5):e595-e602. Depending on the manifestation, SIV, oral pH changes, nutritional deficiencies, and other factors play a role.
Figure 3. Palatal erosion associated with SIV

Source: James Heilman, MD, CC BY-SA 4.0
Dental hard tissues
Dental erosion occurs with AN and BN. Based on a recent systematic review, individuals with ED have a five-fold risk for dental erosion compared to the general population.25Kisely S, Baghaie H, Lalloo R, Johnson NW. Association between poor oral health and eating disorders: systematic review and meta-analysis. Br J Psychiatry 2015;207(4):299-305. Exposure to gastric acid as a result of SIV causes erosion of the palatal surfaces of the maxillary anterior teeth, referred to as perimolysis.25Kisely S, Baghaie H, Lalloo R, Johnson NW. Association between poor oral health and eating disorders: systematic review and meta-analysis. Br J Psychiatry 2015;207(4):299-305. (Figure 3) This condition results in a smooth, glassy surface, loss of tooth structure, and notches along anterior incisal edges as erosion progresses. With long-duration SIV, other surfaces also become affected, with loss of vertical dimension. Among individuals with SIV, almost 70% experience dental erosion.26Uhlen MM, Tveit AB, Stenhagen KR, Mulic A. Self-induced vomiting and dental erosion—a clinical study. BMC Oral Health 2014;29:14:92. Extrinsic acids from foods and drinks, such as citrus fruits, pickles, and diet sodas, also contribute to erosion. Erosive wear reduces the depth of enamel and eventually dentin, resulting in restorations and sealants appearing to be raised.20De Bate R, Tedesco LA, Kerschbaum WE. Knowledge of Oral and Physical Manifestations of Anorexia and Bulimia Nervosa Among Dentists and Dental Hygienists. J Dent Ed 2005;69(3):346-354. Once dentin is exposed, patients may also experience dentin hypersensitivity if the dentinal tubules are open.27Liu XX, Tenenbaum HC, Wilder RS, et al. Pathogenesis, diagnosis and management of dentin hypersensitivity: an evidence-based overview for dental practitioners. BMC Oral Health 2020;20:220. https://doi.org/10.1186/s12903-020-01199-z. Furthermore, a low pH removes the smear layer over dentin, increasing the likelihood of open dentinal tubules.
The findings on increased risk for dental caries in patients with ED are equivocal.19Monda M, Costacurta M, Maffei L, Docimo R. Oral manifestations of eating disorders in adolescent patients. A review. Eur J Paediatr Dent 2021;22(2):155-158. doi: 10.23804/ejpd.2021.22.02.13. Some studies but not others support increases in dental caries, with contributory factors noted to be increases to intake of sugars, changes in salivary flow and poor oral hygiene, hyposalivation associated with vomiting/laxative abuse/use of diuretics and dehydration, and some medications prescribed during treatment for AN and BN.19Monda M, Costacurta M, Maffei L, Docimo R. Oral manifestations of eating disorders in adolescent patients. A review. Eur J Paediatr Dent 2021;22(2):155-158. doi: 10.23804/ejpd.2021.22.02.13. Dehydration and hyposalivation are well-recognized as risk factors for dental erosion, dental caries, several oral mucosal manifestations and halitosis.
Sialadenitis
Sialadenitis (parotid gland enlargement) is a frequent bilateral manifestation in individuals with SIV.
Oral mucosal and peri-oral manifestations
Oral mucosal manifestations are common with AN and BN, including angular cheilitis, atrophic glossitis, labial erythema, oral candidiasis, oral ulcerations and mucositis, gingival bleeding, dry cracked lips, glossodynia (burning tongue), check/lip biting, a yellowish orange discoloration of the soft palate associated with overconsumption of carotenoids, and mucosal trauma.19Monda M, Costacurta M, Maffei L, Docimo R. Oral manifestations of eating disorders in adolescent patients. A review. Eur J Paediatr Dent 2021;22(2):155-158. doi: 10.23804/ejpd.2021.22.02.13.,24Garrido-Martínez P, Domínguez-Gordillo A, Cerero-Lapiedra R, et al. Oral and dental health status in patients with eating disorders in Madrid, Spain. Med Oral Patol Oral Cir Bucal 2019;24(5):e595-e602. SIV is associated with oral ulcerations, oral mucositis, angular cheilitis, labial erythema, and a factor in oral candidiasis.19Monda M, Costacurta M, Maffei L, Docimo R. Oral manifestations of eating disorders in adolescent patients. A review. Eur J Paediatr Dent 2021;22(2):155-158. doi: 10.23804/ejpd.2021.22.02.13.,21Lourenço M, Azevedo Á, Brandão I, Gomes PS. Orofacial manifestations in outpatients with anorexia nervosa and bulimia nervosa focusing on the vomiting behavior. Clin Oral Investig 2018;22(5):1915-1922. doi: 10.1007/s00784-017-2284-y.,23Panico R, Piemonte E, Lazos J, et al. Oral mucosal lesions in anorexia nervosa, bulimia nervosa and EDNOS. J Psychiatr Res 2018;96:178-182.,24Garrido-Martínez P, Domínguez-Gordillo A, Cerero-Lapiedra R, et al. Oral and dental health status in patients with eating disorders in Madrid, Spain. Med Oral Patol Oral Cir Bucal 2019;24(5):e595-e602. Mucosal trauma of the palate, as well as the pharynx and posterior tongue, results from fingers or inanimate objects introduced intraorally for SIV. Nutritional deficiencies are associated with oral candidiasis; atrophic glossitis, glossodynia (vitamin B deficiencies); oral ulcerations (Vit B, folate, and iron deficiencies).7Lo Russo L, Campisi G, Di Fede O, et al. Oral manifestations of eating disorders: a critical review. Oral Dis 2008;14(6):479-484.,28Lamey PJ, Lamb AB. Prospective study of aetiological factors in burning mouth syndrome. Br Med J (Clin Res Ed) 1988:296:1243-1246.,29Frydrych AM, Davies GR, McDermott BM. Eating disorders and oral health: a review of the literature. Aust Dental J 2005;50(1):6-15. In addition, lip and cheek biting are found, associated with psychological and emotional disturbance. With respect to periodontal disease, the findings of studies are equivocal.19Monda M, Costacurta M, Maffei L, Docimo R. Oral manifestations of eating disorders in adolescent patients. A review. Eur J Paediatr Dent 2021;22(2):155-158. doi: 10.23804/ejpd.2021.22.02.13.,20De Bate R, Tedesco LA, Kerschbaum WE. Knowledge of Oral and Physical Manifestations of Anorexia and Bulimia Nervosa Among Dentists and Dental Hygienists. J Dent Ed 2005;69(3):346-354. There is considerable variation for findings on the adequacy of oral hygiene and the influence of nutritional deficiency and host defense mechanisms. However, psychological distress can reduce interest in performing hygiene and oral hygiene, and nutritional deficiencies and resulting blood disorders predispose individuals for periodontal disease.
| Table 3. Oral manifestations of AN and BN |
|---|
| Dental erosion |
| Dentin hypersensitivity |
| Dental caries (equivocal) |
| Halitosis |
| Sialadenitis |
| Oral ulcerations, cheilitis, labial erythema, gingival bleeding, dry cracked lips, lip/cheek biting, yellowish orange discoloration of the soft palate |
| Mucosal trauma of the palate |
| Glossodynia, atrophic glossitis |
| Oral candidiasis |
| Periodontal disease (equivocal) |
Role of Dental Professionals and Interprofessional Collaboration
Dental professionals have an opportunity to identify individuals with AN or BN, and to refer them at an early stage for diagnosis and treatment, since most patients more frequently visit the dental office than they do medical facilities. In 2016, it was reported in Ontario that around 25% of patients with bulimia were first identified during an oral health examination.30College of Dental Hygienists of Ontario. Eating Disorders, August 2016. https://www.cdho.org/Advisories/CDHO_Factsheet_Eating_Disorders.pdf. Early identification is particularly important since early intervention is most effective.31Mirror Mirror. Eating Disorder Statistics. Statistics on Eating Disorders Recovery. https://mirror-mirror.org/facts-staticstics. Additionally, one-fifth of individuals with AN will succumb to associated complications without treatment, while treatment results in a complete recovery in 60% of treated individuals. Patients can be screened and examined for oral manifestations and symptoms associated with AN and BN during routine dental visits. Screening involves a review of the medical history form and patients can be asked to complete a questionnaire. The SCOFF questionnaire is quick to complete, with a positive response to at least 2 questions indicating ED is likely.32Morgan JF, Reid F, Lacey JH. The SCOFF questionnaire: a new screening tool for eating disorders. West J Med 2000;172(3):164-165. doi:10.1136/ewjm.172.3.164. (Table 4) This questionnaire was tested in more than 200 individuals once developed and found to be 100% sensitive in identifying all patients who had ED (n=116), including for bulimic, anorexic, binging and restrictive disorders.32Morgan JF, Reid F, Lacey JH. The SCOFF questionnaire: a new screening tool for eating disorders. West J Med 2000;172(3):164-165. doi:10.1136/ewjm.172.3.164.
| Table 4. SCOFF Questionnaire |
|---|
| 1. Do you make yourself Sick because you feel uncomfortably full? |
| 2. Do you worry that you have lost Control over how much you eat? |
| 3. Have you recently lost more than One stone (14 lb.) in a 3-month period? |
| 4. Do you believe yourself to be Fat when others say you are too thin? |
| 5. Would you say that Food dominates your life? |
Figure 4. Russell’s sign

In addition to oral manifestations, thinning hair and lanugo are obvious provided they are known to be manifestations. Patients typically place their hands on the arms of the dental chair or on their laps. This provides an opportunity to easily observe whether the patient has Russell’s sign. i.e., calluses on the knuckles or back of the hand usually caused by the act of SIV.33Strumia R. Dermatologic signs in patients with eating disorders. Am J Clin Dermatol 2005;6(3):165-173. doi: 10.2165/00128071-200506030-00003. (Figure 4) In some cases, patients may visit for treatment of an associated condition, such as severe dental erosion or dentin hypersensitivity, again providing an opportunity to identify a patient with ED. It is important when having a conversation with patients about potential ED to be diplomatic, empathetic, and nonjudgmental.
While a review of treatment of ED is beyond the scope of this article, the cornerstone is psycho‐behavioral therapy, typically in an ambulatory care setting unless severe, and help from a multi-disciplinary healthcare team.6Hay P. Current approach to eating disorders: a clinical update. Intern Med J 2020;50(1):24-29. doi:10.1111/imj.14691. It has also been suggested that genetic counselling be a component of treatment.9Bulik CM, Blake L, Austin J. Genetics of Eating Disorders: What the Clinician Needs to Know. Psychiatr Clin North Am 2019;42(1):59-73. doi: 10.1016/j.psc.2018.10.007. Other treatment, depending on comorbidities, may include medications, e.g., anti-depressants or anxiolytics, which include dry mouth as a side effect, increasing risk for dental caries and dental erosion.
Beyond identification of individuals with ED, dental professionals provide preventive care and treatment for individuals with ED. Information and advice can be given to patients about dietary acids, information on dental erosion, and the risk to their oral and systemic health. Preventive care including in-office and prescription-level fluorides can be provided to reduce the risk of dental erosion and dental caries along with oral hygiene instructions, and recommendations to manage and prevent oral mucosal lesions. In patients with advanced erosive wear, restorative care will subsequently be required.
Conclusions
AN and BN have increased in prevalence, with a preponderance of females affected. Risk factors are well-recognized, and genetics plays a significant role for both disorders. Dental professionals are in an ideal position to identify individuals suspected of having AN or BN, and to provide timely referrals. In addition, dental professionals provide treatment related to oral manifestations, as well as providing patients with guidance and advice. Interprofessional collaboration increases the likelihood of early intervention which is associated with a higher success rate for treatment.
References
- 1.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, Va: American Psychiatric Association; 2013:338-350.
- 2.World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 11th Revision (ICD‐11). Geneva:World Health Organization; 2019.
- 3.Galmiche M, Déchelotte P, Lambert G, Tavolacci MP. Prevalence of eating disorders over the 2000-2018 period: a systematic literature review. Am J Clin Nutr 2019;109(5):1402-1413. doi: 10.1093/ajcn/nqy342.
- 4.Deloitte Access Economics. The Social and Economic Cost of Eating Disorders in the United States of America: A Report for the Strategic Training Initiative for the Prevention of Eating Disorders and the Academy for Eating Disorders. June 2020. https://www.hsph.harvard.edu/striped/report-economic-costs-of-eating-disorders/.
- 5.National Institute of Mental Health. Eating Disorders. https://www.nimh.nih.gov/health/topics/eating-disorders.
- 6.Hay P. Current approach to eating disorders: a clinical update. Intern Med J 2020;50(1):24-29. doi:10.1111/imj.14691.
- 7.Lo Russo L, Campisi G, Di Fede O, et al. Oral manifestations of eating disorders: a critical review. Oral Dis 2008;14(6):479-484.
- 8.Milosevic A. Eating disorders and the dentist. Br Dent J 1999;186:109-113. https://doi.org/10.1038/sj.bdj.4800036.
- 9.Bulik CM, Blake L, Austin J. Genetics of Eating Disorders: What the Clinician Needs to Know. Psychiatr Clin North Am 2019;42(1):59-73. doi: 10.1016/j.psc.2018.10.007.
- 10.Gaudio S, Quattrocchi CC. Neural basis of a multidimensional model of body image distortion in anorexia nervosa. Neurosci Biobehav Rev 2012;36(8):1839-1847. doi: 10.1016/j.neubiorev.2012.05.003.
- 11.Lulé D, Schulze UME, Bauer K, et al. Anorexia nervosa and its relation to depression, anxiety, alexithymia and emotional processing deficits. Eat Weight Disord 2014;19:209-216.
- 12.Westmoreland P, Krantz MJ, Mehler PS. Medical Complications of Anorexia Nervosa and Bulimia. Am J Med 2016;129(1):30-37. doi: 10.1016/j.amjmed.2015.06.031.
- 13.Mancine RP, Gusfa DW, Moshrefi A, et al. Prevalence of disordered eating in athletes categorized by emphasis on leanness and activity type – a systematic review. J Eat Disord 2020;8:47. https://doi.org/10.1186/s40337-020-00323-2.
- 14.Gaudiani JL, Braverman JM, Mascolo M, Mehler PS. Ophthalmic changes in severe anorexia nervosa: a case series. Int J Eat Disord 2012;45(5):719-721. doi: 10.1002/eat.20970.
- 15.Crow SJ, Peterson CB, Swanson SA, et al. Increased mortality in bulimia nervosa and other eating disorders. Am J Psychiatry 2009;166:1342-1346.
- 16.Lin JA, Woods ER, Bern EM. Common and Emergent Oral and Gastrointestinal Manifestations of Eating Disorders. Gastroenterol Hepatol (NY) 2021;17(4):157-167.
- 17.Ágh T, Kovács G, Supina D, et al. A systematic review of the health-related quality of life and economic burdens of anorexia nervosa, bulimia nervosa, and binge eating disorder. Eat Weight Disord 2016;21(3):353-364. doi:10.1007/s40519-016-0264-x.18.
- 18.Mickley D, Greenfeld D, Quinlan DM, et al. Abnormal liver enzymes in outpatients with eating disorders. Int J Eat Disord 1996;20(3):325-329.
- 19.Monda M, Costacurta M, Maffei L, Docimo R. Oral manifestations of eating disorders in adolescent patients. A review. Eur J Paediatr Dent 2021;22(2):155-158. doi: 10.23804/ejpd.2021.22.02.13.
- 20.De Bate R, Tedesco LA, Kerschbaum WE. Knowledge of Oral and Physical Manifestations of Anorexia and Bulimia Nervosa Among Dentists and Dental Hygienists. J Dent Ed 2005;69(3):346-354.
- 21.Lourenço M, Azevedo Á, Brandão I, Gomes PS. Orofacial manifestations in outpatients with anorexia nervosa and bulimia nervosa focusing on the vomiting behavior. Clin Oral Investig 2018;22(5):1915-1922. doi: 10.1007/s00784-017-2284-y.
- 22.National Eating Disorders Association. Dental complications of eating disorders. nationaleatingdisorders.org/dental-complications-eating-disorders.
- 23.Panico R, Piemonte E, Lazos J, et al. Oral mucosal lesions in anorexia nervosa, bulimia nervosa and EDNOS. J Psychiatr Res 2018;96:178-182.
- 24.Garrido-Martínez P, Domínguez-Gordillo A, Cerero-Lapiedra R, et al. Oral and dental health status in patients with eating disorders in Madrid, Spain. Med Oral Patol Oral Cir Bucal 2019;24(5):e595-e602.
- 25.Kisely S, Baghaie H, Lalloo R, Johnson NW. Association between poor oral health and eating disorders: systematic review and meta-analysis. Br J Psychiatry 2015;207(4):299-305.
- 26.Uhlen MM, Tveit AB, Stenhagen KR, Mulic A. Self-induced vomiting and dental erosion—a clinical study. BMC Oral Health 2014;29:14:92.
- 27.Liu XX, Tenenbaum HC, Wilder RS, et al. Pathogenesis, diagnosis and management of dentin hypersensitivity: an evidence-based overview for dental practitioners. BMC Oral Health 2020;20:220. https://doi.org/10.1186/s12903-020-01199-z.
- 28.Lamey PJ, Lamb AB. Prospective study of aetiological factors in burning mouth syndrome. Br Med J (Clin Res Ed) 1988:296:1243-1246.
- 29.Frydrych AM, Davies GR, McDermott BM. Eating disorders and oral health: a review of the literature. Aust Dental J 2005;50(1):6-15.
- 30.College of Dental Hygienists of Ontario. Eating Disorders, August 2016. https://www.cdho.org/Advisories/CDHO_Factsheet_Eating_Disorders.pdf.
- 31.Mirror Mirror. Eating Disorder Statistics. Statistics on Eating Disorders Recovery. https://mirror-mirror.org/facts-staticstics.
- 32.Morgan JF, Reid F, Lacey JH. The SCOFF questionnaire: a new screening tool for eating disorders. West J Med 2000;172(3):164-165. doi:10.1136/ewjm.172.3.164.
- 33.Strumia R. Dermatologic signs in patients with eating disorders. Am J Clin Dermatol 2005;6(3):165-173. doi: 10.2165/00128071-200506030-00003.