

Introduction
The Holistic Pain Management course strives to assist the dental hygienist in offering support and guidance to the dental patient experiencing pain. The dental hygienist will have obtained knowledge on the experience of pain, appropriate assessment, and evidence-based non-pharmacological interventions for pain. Aiding patients who are experiencing pain is a challenge, however when achieved the results show improvement in their oral health and their overall quality of life, and well-being.1Appukuttan DP. Strategies to manage patients with dental anxiety and dental phobia: literature review. Clin Cosmet Investig Dent. 2016;8:35-50. Published 2016 Mar 10. doi:10.2147/CCIDE.S63626
Role of the Dental Hygienist
The dental hygienist must be able to recognize and be empathetic to a patient's pain as well as have knowledge about the different techniques available to help reduce these symptoms during dental hygiene treatment. This will lead to greater patient trust and cooperation, as well as more productive and effective dental hygiene treatment.2Harlan,K,Wancour, S. An overview of Pain Management,https://www.rdhmag.com/patient-care/radiology/article/16407866/an-overview-of-pain-management. Accessed:December 13, 2022. Dental hygienists play a pivotal role in the assessment, monitoring, interpretation, and evaluation of pain. Effective pain management by dental hygienist is fundamental to quality of care.
THE EXPERIENCE OF PAIN
Fear of pain is strongly associated with anxiety and avoidance of treatment that in turn is highly correlated with increased caries morbidity and DMFS scores.3Farhad Mollashahi N. Adult dental patients with avoidance behaviours. Int J High Risk Behav Addict. 2015;4(1):e23547. Published 2015 Mar 20. doi:10.5812/ijhrba.23547
Pain is a universal experience and an unavoidable part of being human. Pain has a protective function, motivating people to withdraw from damaging or potentially damaging situations and to avoid those same situations in the future. Pain also protects an injured body part while it heals.
Why humans feel pain, what causes pain, the meaning of pain, and how pain can be prevented or reduced has been pondered and discussed throughout history. Pain is the single most common reason people seek medical care.4Chronic Pain and High-impact Chronic Pain Among U.S. Adults, 2019 https://www.cdc.gov/nchs/products/databriefs/db390.htm Accessed: March 10, 2023
What Is Pain?
Pain has been defined as the perceived and unpleasant response to actual or potential tissue damage.5International Association for the Study of Pain. IASP Taxonomy. Revised 2020. www.iasp-pain.org/Taxonomy. Accessed: March 10, 2023 Pain is generally categorized as mild, moderate, or severe. Mild pain is characterized as annoying and nagging; it does not typically impact activities of daily living. Moderate pain is irritating and can impair a person's ability to perform daily activities. Severe pain dominates one's senses, preventing performance of activities of daily living.6Meints SM, Edwards RR. Evaluating psychosocial contributions to chronic pain outcomes. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87(Pt B):168-182.
Traditionally, pain has been considered merely a physical symptom of illness or injury, a simple stimulus-response mechanism. Though the historic role of caregivers has been to relieve pain and suffering, there has been little understanding of the complexity of pain and only limited ways to manage it. Recent research indicates that pain is the net effect of a complex interaction of the ascending and descending nervous systems involving biochemical, physiologic, psychological, and neocortical processes.7Rashid,H (2022)Physiology of pain pathways. Retrieved from https://www.slideshare.net/hassandoc90/physiology-of-pain-pathways
Pain alters the quality of life more than any other health-related problem.8Kawai K, Kawai AT, Wollan P, Yawn BP. Adverse impacts of chronic pain on health-related quality of life, work productivity, depression and anxiety in a community-based study. Fam Pract. 2017;34(6):656-661. It interferes with sleep, mobility, nutrition, thought, sexual activity, emotional well-being, creativity, and self-actualization. Surprisingly, even though pain is such an enormous obstacle to comfort, it is one of the least understood, most undertreated, and often-discounted problems of healthcare providers and their patient’s complaints from pain. With this recent focus on the overprescribing of opioids for pain control, dental hygienist and the entire dental team need to be aware of nonpharmacologic interventions to manage pain.8Kawai K, Kawai AT, Wollan P, Yawn BP. Adverse impacts of chronic pain on health-related quality of life, work productivity, depression and anxiety in a community-based study. Fam Pract. 2017;34(6):656-661.
Who is impacted by pain?
In 2019 the CDC reported that an estimated 50 million Americans (20.4% of the adult population) have experienced chronic pain and that about 20 million of them have “high impact chronic pain” (pain severe enough that it frequently limits the person’s life or work activities). These estimates are based upon the 2016 National Health Interview Survey of over 33,000 adults, which revealed the following:
- Women, unemployed older adults, adults living in poverty, rural residents, and people without some form of public health insurance are significantly more likely to have chronic pain.
- The prevalence of chronic pain and high-impact chronic pain are significantly lower among adults with at least a bachelor’s degree compared with all other education levels.
- Non-Hispanic white adults have a significantly higher age-adjusted prevalence of chronic pain than did all other racial and ethnic subgroups, but there were no significant differences in high-impact chronic pain by race/ethnicity.
- Prevalence of chronic pain was found to be significantly higher among veterans than among nonveterans, but there were no significant differences in the prevalence of high-impact chronic pain.
- Chronic pain contributes to an estimated $560 billion each year in direct medical costs, lost productivity and disability programs.4Chronic Pain and High-impact Chronic Pain Among U.S. Adults, 2019 https://www.cdc.gov/nchs/products/databriefs/db390.htm Accessed: March 10, 2023
PAIN AND THE DENTAL PATIENT
Although dental hygiene treatment is not generally considered to be particularly painful, the findings of a previous study suggest that, at least for some individuals, scaling procedures can result in significant pain.9Lewis, Melba J. Moreland MSN, CCRC; Kohtz, Cindy EdD, MSN, RN, CNE; Emmerling, Sheryl PhD, NEA-BC; Fisher, Mary MA, MSN, RN, NEA-BC; Mcgarvey, Jeremy MS Pain control and nonpharmacologic interventions, Nursing: September 2018 - Volume 48 - Issue 9 - p 65-68 This oral pain accompanied by chronic physical pain is of paramount concern to the dental hygienist. Mobility limitation resulting from neck pain, sciatica or osteoarthritis, particularly in the lower extremities, makes it difficult for those affected to visit dental offices for routine dental hygiene treatment.
With tight patient schedules, emergencies, and productivity goals to consider, it is easy to overlook proper patient positioning for a patient experiencing chronic pain and body aches. However, taking the time to position the patient, dental hygienist and equipment properly can not only have positive ramifications for the operator’s posture, comfort, and career longevity — it can also lead to better treatment and increased productivity.10Sullivan MJ, Neish N. The effects of disclosure on pain during dental hygiene treatment: the moderating role of catastrophizing. Pain. 1999;79(2-3):155-163. doi:10.1016/s0304-3959(98)00163-8.
Communication with patient regarding pain
One of the most essential aspects of mastering effective, individually tailored pain management is the ability to clearly communicate with the dental patient. Listening is also a form of communication that is often overlooked in clinical practice. Acknowledging and listening to the concerns of patients demonstrate the clinician’s genuine interest in patient-centered care. Studies have shown that patients not only favor providers who take the time to listen, good communication also supports effective patient care regarding pain management. There is an aspect of empathetic listening that needs to occur between the dental hygienist and the patient regarding pain management prior to treatment. This is a collaborative effort that helps the patient to be more comfortable and dental hygienist to render more effective dental hygiene treatment.11Positioning for success.https://www.rdhmag.com/career-profession/students/article/16405973/positioning-for-success. January 1, 2012. Accessed: August 1, 2021
Origin of Pain
Physiology of Pain
Pain derives from the central nervous system to include the brain and the spinal cord. The two form the central nervous system while the sensory motor nerves compose the peripheral nervous system. The brain and spinal cord are the center of the system, and the sensory and motor nerves reach the rest of the body. The sensory nerves send the message back to the brain via the spinal cord. When an injury occurs, the multitude of nerve fibers respond by producing chemical responses, which determines how sensations are interpreted.12Brady, M.,Alvear,B, Meeting Patient’s Pain Management Needs, Special Edition- Dimensions of Dental Hygiene, March 2021;19(3):16, 18, 21.
PAIN CATEGORIES
The three pain categories are described as mild, moderate, or severe.
Mild - Annoying and nagging; it does not typically impact activities of daily living.
Moderate -Irritating and can impair the person’s ability to perform activities of daily living.
Severe Dominates one’s sense, preventing performance of activities of daily living.5International Association for the Study of Pain. IASP Taxonomy. Revised 2020. www.iasp-pain.org/Taxonomy. Accessed: March 10, 2023
DURATION OF PAIN
Acute and chronic pain are different clinical entities. Acute pain is provoked by a specific disease or injury, serves a useful biologic purpose, is associated with skeletal muscle spasm and sympathetic nervous system activation, and is self-limited. Chronic pain, by contrast, may be considered a disease state. It is pain that outlasts the normal time of healing, if associated with a disease or injury. Chronic pain may arise from psychological states, serves no biologic purpose, and has no recognizable endpoint.13Khera T, Rangasamy V. Cognition and Pain: A Review. Front Psychol. 2021;12:673962. Published 2021 May 21. doi:10.3389/fpsyg.2021.67396214Orhurhu VJ, Roberts JS, Ly N, et al. Ketamine In Acute and Chronic Pain Management. Updated : 2022 Sep 19. StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539824/
Acute Pain
Dental professionals are well acquainted with patients with acute pain. This is the patient who presents him/herself in excruciating pain from experiencing an avulsed tooth, periodontal abscess, or a cracked tooth. Acute pain is caused by noxious stimulation due to injury, a disease process, or the abnormal function of muscle or viscera. Acute pain begins suddenly, is usually sharp in quality and correlates with the amount of damage. It is temporary and subsides as healing takes place. In acute pain, the central nervous system is intact and acute pain is a symptom.15Doody O, Bailey ME. Understanding pain physiology and its application to person with intellectual disability. J Intellect Disabil. 2019;23(1):5-18. doi:10.1177/1744629517708680 Psychological effects of unrelieved pain can lead to anxiety and depression, and unrelieved acute pain may lead to chronic pain.6Meints SM, Edwards RR. Evaluating psychosocial contributions to chronic pain outcomes. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87(Pt B):168-182.16Quinlan, Jane FRCA, FFPMRCA,; Cox, Felicia FRCN. Acute pain management in patients with drug dependence syndrome. PAIN Reports 2(4):p e611, July/August 2017.
Chronic Pain
Chronic pain is pain that persists, recurs, or progresses over a long period of time and is often resistant to medical treatments. The nature of chronic pain can mean that in some instances, it is ongoing and constant. This makes the person who has chronic pain more susceptible to psychological consequences, including depression and anxiety, and this psychological distress can in turn increase the pain.17Sheng J, Liu S, Wang Y, Cui R, Zhang X. The Link between Depression and Chronic Pain: Neural Mechanisms in the Brain. Neural Plast. 2017;2017:9724371. doi:10.1155/2017/9724371
Some chronic pain that can have impact on a patient’s dental hygiene treatment includes, chronic low back pain, which impacts how long a patient may comfortably sit in the dental chair, and arthritis in the hands and fingers, which may significantly affect a patient’s manual dexterity when grasping oral care products. The usual symptoms are pain and stiffness accompanied by loss of function.18Mills SEE, Nicolson KP, Smith BH. Chronic pain: a review of its epidemiology and associated factors in population-based studies. Br J Anaesth. 2019;123(2):e273-e283. doi:10.1016/j.bja.2019.03.023
What causes pain
The causes of pain are divided into the categories of nociceptor, neuropathic, psychogenic, and idiopathic.14Orhurhu VJ, Roberts JS, Ly N, et al. Ketamine In Acute and Chronic Pain Management. Updated : 2022 Sep 19. StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539824/
Nociceptor Pain
Nociceptor pain is acute pain that results when tissue damage produces a stimulus that sends an electrical impulse across a receptor (nociceptor) by way of a nerve fiber leading to the central nervous system.
Nociceptor pain is usually acute, well-localized, sharp, worsens with movement, accompanied by inflammation and it is usually caused by trauma or injury to the area. Intraoral burns to the oral mucosa from eating very hot food is an example of nociceptor pain.20Tan HL, Smith JG, Hoffmann J, Renton T. A systematic review of treatment for patients with burning mouth syndrome. Cephalalgia. 2022;42(2):128-161. doi:10.1177/03331024211036152
Neuropathic Pain
Neuropathic pain is caused by a primary lesion or dysfunction within the nervous system itself. Unlike nociceptive pain, neuropathic pain is most often classified as chronic pain, which may increase in intensity over time. Temporomandibular joint pain is an example of neuropathic pain.21Brody, A., Novel Therapy May Relieve Temporomandibular Joint Pain, https://dimensionsofdentalhygiene.com/novel-therapy-may-relieve-temporomandibular-joint-pain/ Accessed: January 18, 2023.
Oral pain due to cancer and associated treatments is common. The prevalence and severity of oral cancer is high. Painful oral mucositis develops in head and neck cancer patients following surgery and associated radiation therapy and/or chemotherapy. In addition, oral pain, including from mucositis, occurs in patients receiving chemotherapy for cancers of the hematopoietic system and cancers at other anatomic sites. Despite pain management practices that include high-dose opioid analgesics, patients rarely obtain relief from either head and neck cancer or mucositis pain because oral pain in cancer patients is likely due to both nociceptive and neuropathic pain. Effective management of pain requires treatments for both processes.22Epstein JB, Miaskowski C. Oral Pain in the Cancer Patient. J Natl Cancer Inst Monogr. 2019;2019(53):lgz003. doi:10.1093/jncimonographs/lgz003
Psychogenic Pain
Psychogenic pain is believed to be sustained mainly by psychological factors. It does not refer to the common idea that pain experienced by some patients is exacerbated by psychological factors, or the finding of high pain-related distress or comorbid psychiatric disease. Instead, it implies that the pain is best understood because of psychological processes. It is classified as a somatic symptom disorder with prominent pain, which is diagnosed based on excessive thoughts, feelings, or behaviors related to pain that are distressing, impair function, and appear out of proportion to physical findings. It must be remembered that psychogenic pain is truly experienced and is not a deception.23Riggs A, Breuer B, Patel V, et al. Pain-related distress among patients referred to a community-based palliative care program. Palliat Support Care. 2019;17(3):338-344. An example of psychogenic pain is the complaint of occlusal discomfort when there is no clinical evidence of deviation or trauma to a patient’s occlusion. The patient may complain of constant discomfort despite treatment to eliminate the pain. In addition to having difficulty describing location, quality, and depth of pain.24Toyofuku A. Psychosomatic problems in dentistry. Biopsychosoc Med. 2016;10:14. Published 2016 Apr 30. doi:10.1186/s13030-016-0068-2
Idiopathic Pain
Idiopathic pain exists without underlying neural or tissue damage. Idiopathic pain is diverse and can be described as burning, itching, stinging, irritating, stabbing, and/or sharp. Burning Mouth Syndrome can be categorized as idiopathic.25Schramm E, Waisman A. Microglia as Central Protagonists in the Chronic Stress Response. Neurol Neuroimmunol Neuroinflamm. 2022;9(6):e200023. Published 2022 Sep 7. doi:10.1212/NXI.0000000000200023 Idiopathic pain is characterized by a state of pain amplification, psychological distress, and enhanced inflammation. Depression and anxiety are often associated with idiopathic pain.
Pain Threshold and Pain Tolerance Defined
Pain threshold refers to the lowest intensity at which a given stimulus is perceived as painful. Pain tolerance is the greatest level of pain that one is able to endure.25Schramm E, Waisman A. Microglia as Central Protagonists in the Chronic Stress Response. Neurol Neuroimmunol Neuroinflamm. 2022;9(6):e200023. Published 2022 Sep 7. doi:10.1212/NXI.0000000000200023
Influence of Pain Threshold
The experience of pain is influenced by both physiologic and psychosocial factors, all of which dental hygienist must consider in developing pain management interventions.
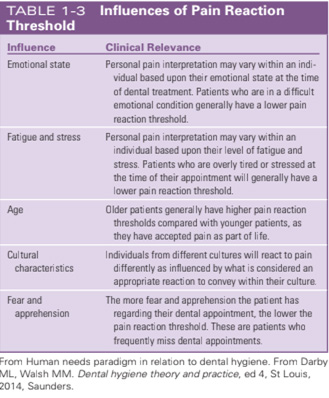
Emotional State
Pain and stress are both adaptive in protecting the body. However, if either of the two processes become chronic; it can lead to long-term maladaptive changes in physiology and, consequently, behavior resulting in compromised well-being. Some patients are more sensitive and reactive to stress, and others are more resilient. Studies have found that decreased pain modulation occurred only among those who have a high stress responsiveness, and increased pain adaptation occurred only among those who have low stress responsiveness.26Geva N, Defrin R. Opposite Effects of Stress on Pain Modulation Depend on the Magnitude of Individual Stress Response. J Pain. 2018 Apr;19(4):360-371. doi:10.1016/j.jpain.2017.11.01127Abdallah CG, Geha P. Chronic Pain and Chronic Stress: Two Sides of the Same Coin?. Chronic Stress (Thousand Oaks). 2017;1:2470547017704763. doi:10.1177/2470547017704763
Fatigue and Stress
Emotional distress is commonly observed in people with chronic pain. Anxiety is common for patients with pain. Up to 45% of patients with chronic pain screen positive for anxiety disorder.28Sullivan MD, Ballantyne JC. Must we reduce pain intensity to treat chronic pain?. Pain. 2016;157(1):65-69. doi:10.1097/j.pain.0000000000000336 Up to 50% of patients with chronic pain experience depression, and on average, 65% of depressed individuals also report pain symptoms. There is evidence of a strong association between chronic pain and depression, but evidence is lacking as to whether chronic pain causes depression or depression causes chronic pain.29Sullivan MD, Ballantyne JC. When Physical and Social Pain Coexist: Insights Into Opioid Therapy. Ann Fam Med. 2021;19(1):79-82. doi:10.1370/afm.2591 Dental hygienists must take into consideration the patient’s level of anxiety during treatment. Addressing a patient’s anxiety and being empathetic will alleviate a patient’s anxiety level during dental hygiene treatment.
Age
There is a consistent positive relationship between age and the experience of chronic pain and there is increased frequency, severity, impact, and anatomic distribution of persistent pain associated with aging. Aging, however, has no strong effect on pain tolerance. Clear evidence exists that there is a high prevalence of chronic pain in the older adult, and this can be attributed partly to the physiologic changes of the peripheral and central pain mechanisms.30Domenichiello AF, Ramsden CE. The silent epidemic of chronic pain in older adults. Prog Neuropsychopharmacol Biol Psychiatry. 2019 Jul 13; 93:284-290. doi:10.1016/j.pnpbp.2019.04.006
Studies have shown a significant gender-related difference in pain perception and responses, suggesting that women are more sensitive to noxious stimuli than men and experience pain more often and of higher intensity and longer duration. In addition, brain imaging has shown sex-related differences concerning the spatial distribution and magnitude of acute pain responses.31Geva N, Golan S, Pinchas L, Defrin R. Sex effects in the interaction of acute stress and pain perception. Pain. 2023;164(3):587-597. doi:10.1097/j.pain.0000000000002743
It has been found that the differences between males and females regarding sensitivity to pain is affected by psychological factors such as anxiety, which is more associated with pain in males. Men and women are both susceptible to pain after surgery, but postsurgical pain is more intense in women than in men, men are more troubled by low and persistent levels of pain.32Keogh E. Sex and Gender Differences in Pain Across the Life Course. Handbook of Pain and Palliative Care 2018. Doi : 10.1007/978-3-319-95369-4_18
Culture
Many cultures also have distinct cultural beliefs regarding the meaning, origin, and role of pain, which can affect how a patient interprets and perceives pain.33Hasenfratz K, Moergeli H, Sprott H, Ljutow A, Hefti R, Rittmayer I, Peng-Keller S and Rufer M (2021) Do Chronic Pain Patients Wish Spiritual Aspects to Be Integrated in Their Medical Treatment? A Cross-Sectional Study of Multiple Facilities. Front. Psychiatry 12:685158. Each cultural and social group has its own unique language of pain and distress, its own complex expressions by which ill or unhappy people make other people aware of their suffering. There is a specific, often standardized way of signaling both verbally and non-verbally, that the person is in pain or discomfort. The form that this pain behavior takes is largely culturally determined, as is the response to this behavior. This depends on factors such as whether the patient’s culture values or does not value the display of emotions, body language or verbal expression in response to pain or injury. Some cultural groups expect an extravagant display of emotion in the presence of pain, but others value stoicism, restraint and playing down the pain.34Sharma S, Abbott JH, Jensen MP. Why clinicians should consider the role of culture in chronic pain. Braz J Phys Ther. 2018;22(5):345-346. For example, Hispanics have been known to verbally express their pain. This is termed as being emotive. Whereas Asians, are considered stoic in their expression of pain.35Carteret,M. https://www.dimensionsofculture.com/2010/11/cultural-aspects-of-pain-management/ Accessed: April 1,2022 It has also been observed that having a provider who speaks the patient’s native language is also critical for communicating pain.
Fear and Apprehension
It is very common to have patients say, “I have not been to the dentist for a while because I am afraid of the pain.” Some patients may create scenarios of pain worse than the actual experience of pain. This is known as pain catastrophizing, which is an exaggerated, negative cognitive and emotional orientation toward actual or anticipated pain experiences. Catastrophizing has been associated with an increased perception of severity and disability in both acute and chronic pain among persons with many different pain diagnoses. Catastrophizing also alters perception of noxious stimulation.36Simon, E., Zsidó, A.N., Birkás, B. et al. Pain catastrophizing, pain sensitivity and fear of pain are associated with early life environmental unpredictability: a path model approach. BMC Psychol 10, 97 (2022).
People who experience chronic pain often anticipate that specific activities will increase pain or induce further injury, and these fears may contribute to avoidance of activity and subsequently leading to greater physical deconditioning, emotional distress, and ultimately, greater disability.28Sullivan MD, Ballantyne JC. Must we reduce pain intensity to treat chronic pain?. Pain. 2016;157(1):65-69. doi:10.1097/j.pain.0000000000000336
Low Health Literacy and Pain
The impact of health literacy on health status and health outcomes is receiving more and more attention. A study was conducted in 2018 to evaluate the association of health literacy with chronic pain intensity and pain perception. The study concluded that individuals with a higher level of health literacy experienced less pain intensity, which seemed to be caused by better pain management; therefore, supporting the development of health literacy in patients with chronic pain could be seen as an important objective of integrated care.37Köppen PJ, Dorner TE, Stein KV, Simon J, Crevenna R. Health literacy, pain intensity and pain perception in patients with chronic pain. Wien Klin Wochenschr. 2018 Jan;130(1-2):23-30. doi:10.1007/s00508-017-1309-5 This also includes a person’s beliefs and knowledge about pain.
Lack of understanding pain leads to anxiety, excessive worrying, emotional instability, sensitivity, and may serve to influence pain stimulus appraisal or threat of a potential pain stimulus. Such personality traits may even reduce the threshold at which pain is perceived as threatening and at which point pain elicits catastrophic thoughts.38Banozic A, Miljkovic A, Bras M, Puljak L, Kolcic I, Hayward C, Polasek O. Neuroticism and pain catastrophizing aggravate response to pain in healthy adults: an experimental study. Korean J Pain. 2018 Jan;31(1):16-26. doi:10.3344/kjp.2018.31.1.16
ASSESSING PAIN
Medical History
The first step in the dental hygiene process of care is assessment. This phase involves collecting and analyzing patients’ health information and clinical data to provide comprehensive and adequate care. An essential part of the assessment phase is the medical history, also known as a personal health record or health history. The primary purpose of medical history is to obtain and document information about patients’ past and present history of medical conditions and diseases, as well as to identify risk factors for oral disease and systemic conditions. Medical history can be obtained through a self-administered questionnaire, or an interview conducted by the dental hygienist. Regardless of how the medical history is obtained, it is important to document all information clearly and concisely regarding signs, symptoms, medical conditions, and other risk factors in chronological order.39Castellanos, S., Dental Hygiene Approach Toward COVID-19, Dimensions of Dental Hygiene,February 2021, pgs.40-43.
Relevant past medical history includes:
- Prior medical and current illnesses or conditions and previous surgeries
- Prior psychiatric illnesses
- Prior surgeries, scarring, repeated surgeries (may increase sensitivity to pain)
- Past injuries and accidents
- Coexisting acute or chronic illnesses
- Chemical dependence
- Prior problems with pain and treatment outcomes
A precise and systematic assessment of pain is important for making an accurate diagnosis and for the development of an effective treatment plan. Pain is a multidimensional phenomenon that produces strong emotional reactions which can affect an individual’s function, quality of life, emotional state, social and vocational status, and general well-being. Therefore, it is recommended that pain be assessed using a multidimensional approach and that these various impacts be addressed and included in the diagnostic formulation. A comprehensive pain assessment includes a history of the pain, behavioral observations, past medical history, medications, family history, a physical examination, and if necessary, diagnostic testing.40Swann M. Recognising the importance of language in effective pain assessment. Nurs Stand. 2021;36(2):43-50. doi:10.7748/ns.2021.e11563
Pain History
A pain assessment begins with the history of the problem and can be obtained from written documents and from interviews with the person in pain as well as family members and other caregivers. Pain is a subjective symptom and pain assessment is, therefore, based on the patient’s own perception of pain and its severity.
Questions to Ask When Assessing Pain
When obtaining a pain history, the mnemonic SOCRATES can be useful:
- Site – Where is the pain?
- Onset – When did it start?
- Character – Can you describe the pain?
- Radiation – Does the pain spread anywhere?
- Associations – Are there other problems associated with the pain?
- Time course – Does the pain follow any pattern? How long does it last?
- Exacerbating or relieving factors – Does anything worsen or improve it?
- Severity – How bad is the pain?41Timmerman A, Parashos P. Management of dental pain in primary care. Aust Prescr. 2020;43(2):39-44. doi:10.18773/austprescr.2020.010
Answers to these questions should be noted in patient progress notes. Clinicians should incorporate these comments into the patient’s overall treatment plan.
IMPACT OF PAIN IN ACTIVITIES OF DAILY LIVING
Some organizations, however, are abandoning pain-rating scales and instead assessing patients by asking how much their function is impaired and how much time they are spending in bed because of pain. This kind of assessment allows a patient to better articulate pain levels and gives the provider more insight into how the patient’s pain in affecting day-to-day living, providing an ability to create a more effective treatment plan.42Guidetti S, Nielsen KT, von Bülow C, Sampedro-Pilegaard M,Klokker, L,Waehrens,E E, Evaluation of an intervention programme addressing ability to perform activities of daily living among persons with chronic conditions: study protocol for a feasibility trial (ABLE) BMJ Open 2018;8:e020812. doi: 10.1136/bmjopen-2017-02081243Edemekong PF, Bomgaars DL, Sukumaran S, Schoo C. Activities of Daily Living. In: StatPearls. Treasure Island (FL): StatPearls Publishing; November 19, 2022.
The Activities of Daily Living (ADL) are skills required to manage one’s basic physical needs. The basic ADL includes the following categories: Ambulating: The extent of an individual’s ability to move from one position to another and walk independently. Feeding: The ability of a person to feed oneself. Dressing: The ability to select appropriate clothes and to put the clothes on. Personal hygiene: The ability to bathe and groom oneself and maintain dental hygiene, nail, and hair care. Continence: The ability to control bladder and bowel function Toileting: The ability to get to and from the toilet, using it appropriately, and cleaning oneself.43Edemekong PF, Bomgaars DL, Sukumaran S, Schoo C. Activities of Daily Living. In: StatPearls. Treasure Island (FL): StatPearls Publishing; November 19, 2022. Pain can seriously impact these activities.
Behavioral Observations
Most people who are experiencing pain usually demonstrate it either by verbal complaint or nonverbal behaviors or indicators. It is important, however, to remember that people in pain may or may not display behaviors that are considered an indication of being in pain and making judgments about their honesty are inappropriate.
Psychosocial History
In a dental setting, it is not the norm to inquire into past or current developmental, marital, or vocational problems, stressors or depressive symptoms, and reinforcers of the pain (e.g., compensation/litigation issues) The clinician must be aware that these factors may also contribute to exacerbating pain. A systematic, targeted, pain-focused physical examination is most fruitful when the pain history interview and behavioral observations are conducted at the same time.
General inspection
This begins when the clinician first encounters the patient and notes any obvious sign of pain, such as limping, unusual posture of the body, splinting or guarding, facial expression, vocalizations, and the presence of obesity.
Sleep
Areas that are of concern include perceived pain-related disability, emotional distress (e.g., depression, anxiety), and sleep disturbance.44Berggren K, Broström A, Firestone A, Wright B, Josefsson E, Lindmark U. Oral health problems linked to obstructive sleep apnea are not always recognized within dental care-As described by dental professionals. Clin Exp Dent Res. 2022;8(1):84-95.
Substance Abuse
Due to the significant prevalence of alcohol/substance use and prescription opioid misuse among persons with chronic pain, a comprehensive screening is generally indicated. When symptom exaggeration or malingering is suspected, it is important to consider that it may occur because of psychological processes or environmental factors that shape the person’s response to pain.45Wachholtz A, Robinson D, Epstein E. Developing a novel treatment for patients with chronic pain and Opioid User Disorder. Subst Abuse Treat Prev Policy. 2022;17(1):35. Published 2022 May 7. doi:10.1186/s13011-022-00464-4
Accommodating a Patient in Pain During the Dental Hygiene Appointment.
Providing dental care to patients with pain may require modifications to the traditional treatment plan. Dental hygienists need to be prepared to accommodate patients in pain. Dental hygienists need to determine if patients can transfer to the dental chair by themselves or with the help of a caregiver and/or sliding block. If the patient is in a wheelchair, the armrest on the dental chair should be removed, and the chair should be at the level of the wheelchair or slightly lower. The rheostat pedal, headlight, and any hoses should also be cleared for the transfer.46Singh, N.,Providing Care to Patients with Special Needs Dimensions of Dental Hygiene. July/August 2019;17(7):46–49. Accessed: March 1, 2023. If the dental team will assist in the transfer, members must be properly trained to ensure patient safety and prevent falls. Once the patient is seated, he or she will need to be positioned, centered, and reclined for treatment. Extra pillows, cushions, and support pads can be used to keep the patient comfortable. Treatment may need to stop periodically to allow the patient to reposition if he or she starts to lose muscle control.47Shirley Musich, Shaohung S. Wang, Joann Ruiz, Kevin Hawkins, Ellen Wicker, The impact of mobility limitations on health outcomes among older adults, Geriatric Nursing, Volume 39, Issue 2, 2018, Pages 162-169,
Dental hygienists need to be attentive to the pain needs of this patient population, beginning with the initial greeting and continuing through the completion of the appointment.
Behavioral management techniques used in pediatric dentistry such as Tell-Show-Do, can often be applied to individuals experiencing chronic pain. Throughout the procedure, the dental hygienist should provide positive reinforcement. Depending on the patient’s pain level, instructions might have to be repeated several times.
Stabilization of the patient’s head can be accomplished with pillows, rolled blankets, or towels. The patient’s head needs to be raised slightly to avoid compromising the neck. Patients experiencing TMJ pain, during treatment can achieve oral stabilization via mouth props such as rubber or Styrofoam bite blocks (with floss tied through one end to prevent patient aspiration), disposable bite sticks (made of tongue depressors and gauze), cotton rolls, and rolled gauze.48Moore, T., Dental Care for Patients with Special Needs, Decisions in Dentistry. September 2016;2(09):50–53. Accessed: March 1, 2023.
Preventive Counseling for Patients with Pain
Many people with disabling osteoarthritis, rheumatoid arthritis, and other conditions have difficulty practicing good oral hygiene and traveling to dental offices for professional help. Various inexpensive measures can help such individuals, including education of their caregivers and provision of antimicrobial mouthwashes and special toothbrushes. Also helpful would be such simple and inexpensive measures as providing antimicrobial mouthwashes and high-fluoride toothpastes and mouth rinses to patients with limited manual dexterity. Mouthwashes containing chlorhexidine may be especially useful in helping to control plaque accumulation when mechanical oral hygiene practices are not feasible. Electric or other special toothbrushes can be provided to those afflicted with impairments of their hands and upper extremities. Such measures would enable them to maintain better oral hygiene even without professional intervention. Sonic and ultrasonic toothbrushes may be advantageous in decreasing plaque and gingival bleeding in individuals whose hand function is limited.49Janto M, Iurcov R, Daina CM, Neculoiu DC, Venter AC, Badau D, Cotovanu A, Negrau M, Suteu CL, Sabau M, Daina LG. Oral Health among Elderly, Impact on Life Quality, Access of Elderly Patients to Oral Health Services and Methods to Improve Oral Health: A Narrative Review. Journal of Personalized Medicine. 2022; 12(3):372.
Patients whose hands or fingers are affected by pain may exhibit poor oral hygiene due to difficulty in performing self-care. Clinicians can modify self-care devices to improve the effectiveness of oral hygiene regimens. For patients who have difficulty grasping, the use of a wide-handled power toothbrush is recommended. The addition of bicycle grips, tennis balls or soft plastic toothbrush handles may also make them easier to hold. An extender (ruler, rod, or wooden spoon) can be taped to the handle of a toothbrush to aid patients with a limited range of motion. Caregivers should also receive counseling on the importance of oral health, the oral/systemic link, optimal nutrition, and oral hygiene techniques so they can help patients maintain their oral health.48Moore, T., Dental Care for Patients with Special Needs, Decisions in Dentistry. September 2016;2(09):50–53. Accessed: March 1, 2023. Routine dental hygiene appointments help to motivate patients to adhere to the oral care protocols to prevent disease.
Evidence-based Nonpharmacologic Therapies
Evidence-based nonpharmacologic therapies are safe when correctly administered and can be effective components of comprehensive pain management that can reduce the need for opioids. Nonpharmacologic therapies can be the sole intervention, or they can be combined with other treatments. Nonpharmacologic interventions include physical, psychological, and mind-body modalities. These therapies should be used in consultation with a physician or physical therapist for optimum effectiveness.
PHYSICAL MODALITIES
Heat is effective for mostly dull and persistent pain associated with stiffness, cramping, and neuropathic sensitivity. Muscle pain responds well to heat, which also promotes relaxation and comfort. Superficial heat can be applied using wet or dry hot packs, heat wraps, hot baths and saunas. These mechanisms serve to reduce muscle tonicity and relax muscles, thereby reducing spasms and musculoskeletal pain and increasing muscle flexibility.50Freiwald J, Magni A, Fanlo-Mazas P, Paulino E, Sequeira de Medeiros L, Moretti B, Schleip R, Solarino G. A Role for Superficial Heat Therapy in the Management of Non-Specific, Mild-to-Moderate Low Back Pain in Current Clinical Practice: A Narrative Review. Life. 2021. It would be beneficial to keep a heating pad for patients to use during dental hygiene treatment if necessary.
Massage is the use of touch on specific areas and tissues for therapeutic purposes. Therapeutic massage involves the application of hands or elbows with the intention of solving a physical problem. Research supports the benefits of massage therapy for pain management, decreasing anxiety and depression, and reducing pain intensity in patients undergoing surgical procedures. Massage reduces pain by stimulating A-beta fibers, resulting in closing of the “gate” to impulses from the periphery, additionally massages stimulate the release of endorphins.51D’Arro, C. (2018). Mindful Dentist. The International Journal of Whole Person Care, 5(2). https://doi.org/10.26443/ijwpc.v5i2.182
Acupuncture, which is a mainstay in the healthcare practices of traditional Chinese medicine, is commonly used for the treatment of pain. There is substantial evidence for acupuncture being effective in the treatment of acute and chronic pain.52Xu, Jianghan BS; Wu, Boyi BS; Xie, Shengji BS; Wu, Guanghui BS; Zhang, Heng BS; Fu, Yangyang MM; Guo, Guangxin MD,. Effectiveness and safety of massage for chronic pain in patients with knee osteoarthritis: A protocol for systematic review and meta-analysis. Medicine 101(3):p e28533, January 21, 2022.
PSYCHOLOGICAL MODALITIES
Cognitive-Behavioral Therapy (CBT)
Cognitive-behavioral therapy (CBT), a form of psychotherapy, has recently been applied to patients with chronic pain. Several studies have found that, whether administered alone or in combination with medical treatment, CBT improved pain and related problems.53Xiang A, Cheng K, Shen X, Xu P, Liu S. The Immediate Analgesic Effect of Acupuncture for Pain: A Systematic Review and Meta-Analysis. Evid Based Complement Alternat Med. 2017;2017:3837194. doi:10.1155/2017/3837194
MIND-BODY TECHNIQUES
Mindfulness-Based Interventions
The goal of mindfulness meditation is not to eliminate pain or anxiety but rather to get patients to focus on breathing and relaxation techniques (focused awareness). Patients are taught to achieve nonjudgmental self-acceptance and to focus the mind on the present moment.54Lim JA, Choi SH, Lee WJ, et al. Cognitive-behavioral therapy for patients with chronic pain: Implications of gender differences in empathy. Medicine (Baltimore). 2018;97(23):e10867. doi:10.1097/MD.0000000000010867
Relaxation Therapies
There are several different types of relaxation techniques, like meditation, breathing techniques, visualization, autogenic training, and progressive muscle relaxation. One possible explanation of why relaxation techniques relieve chronic pain, is that chronic pain is maintained and increased by psychological stress and physical tensions. It has been estimated that three months of regular relaxation practice is necessary to obtain pain reduction. The effect of relaxation techniques will depend on the individual and the type of chronic pain.55Vambheim SM, Kyllo TM, Hegland S, Bystad M. Relaxation techniques as an intervention for chronic pain: A systematic review of randomized controlled trials. Heliyon. 2021;7(8):e07837. Published 2021 Aug 20. doi:10.1016/j.heliyon.2021.e07837
Distraction Intervention
Distraction is shifting attention away from pain or painful stimuli to something more engaging or enjoyable. Distraction intervention is defined as a cognitive or behavioral strategy to relieve pain, stress, and anxiety by distracting patients from a harmful stimulus to what they do or something attractive through a non-pharmacological method of pain management.56Cho MK, Choi MY. Effect of Distraction Intervention for Needle-Related Pain and Distress in Children: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2021;18(17):9159. Published 2021 Aug 31. doi:10.3390/ijerph18179159
Yoga
Yoga is a mind-body and exercise practice that helps relieve chronic pain. Yoga has many of the same benefits as mindfulness practice due to the common focus on breath, body, and present-moment awareness. There are different types of yoga, with the most evidence of benefit being shown through Iyengar yoga, hatha yoga, and Viniyoga. It is not fully understood how yoga helps with pain, but emerging evidence suggests it might help people more effectively control how they think and feel, both mentally and physically. It may also work by improving muscle flexibility, promoting relaxation, reducing inflammation or increasing the release of pain-relieving endorphins. The effects of yoga have been found to be roughly equivalent to cognitive behavioral therapy. A meta-analysis of 17 studies concluded that yoga could improve daily function among people with fibromyalgia, migraine, low back pain, and many other types of chronic pain conditions. It is recommended by the American Pain Society for people with low back pain does not improve with other self-care strategies.57Wieland LS, Skoetz N, Pilkington K, Harbin S, Vempati R, Berman BM. Yoga for chronic non-specific low back pain. Cochrane Database Syst Rev. 2022;11(11):CD010671. Published 2022 Nov 18.
Evaluating the Effectiveness of Interventions
Outcome evaluation is one of the most critical phases of pain management. If the expected outcome is pain reduction; outcome evaluation identifies its success or failure. It also identifies how much the pain has been reduced, how long it has taken, and long-term effects of the treatment.
CONSEQUENCES OF UNTREATED/UNDERTREATED PAIN
Common consequences of untreated chronic pain include decreased mobility, impaired immunity, decreased concentration, anorexia, and sleep disturbances. In addition, researchers have found that chronic pain in older adults accelerates memory decline, increases the probability of developing dementia, and increases the risk of mortality by 29%.58Whitlock EL, Diaz-Ramirez LG, Glymour MM, Boscardin WJ, Covinsky KE, Smith AK. Association Between Persistent Pain and Memory Decline and Dementia in a Longitudinal Cohort of Elders. JAMA Intern Med. 2017 Aug 1;177(8):1146-1153
DENTAL STANDARDS OF CARE
Standards of care for dental hygienists in the management of pain include, but are not limited to:
- Acknowledging and accepting the patient’s pain.
- Identifying the most likely source of the pain.
- Assessing pain at regular intervals, including each new complaint of pain, utilizing a pain assessment tool.
- Assessing barriers to effective pain management.
- Reporting the patient’s level of pain and developing a plan of care that includes interdisciplinary input.
- Advocating for the patient and family for effective pain management.
- Educating patient, family, and significant others on:
- Their role in pain management plan and expected outcomes
- Detrimental effects of unrelieved pain
- Overcoming barriers to effective pain management
Conclusion
It is imperative that dental hygienist understand their role in managing pain as one of their primary obligations and responsibilities. It is the duty of all involved in caring for patients in pain to do everything possible to bring them relief. To do less is to fail to provide quality patient care. To best carry out this responsibility, it is necessary for all professionals to continue to expand their knowledge and skills in managing this crucial healthcare issue.
References
- 1.Appukuttan DP. Strategies to manage patients with dental anxiety and dental phobia: literature review. Clin Cosmet Investig Dent. 2016;8:35-50. Published 2016 Mar 10. doi:10.2147/CCIDE.S63626
- 2.Harlan,K,Wancour, S. An overview of Pain Management,https://www.rdhmag.com/patient-care/radiology/article/16407866/an-overview-of-pain-management. Accessed:December 13, 2022.
- 3.Farhad Mollashahi N. Adult dental patients with avoidance behaviours. Int J High Risk Behav Addict. 2015;4(1):e23547. Published 2015 Mar 20. doi:10.5812/ijhrba.23547
- 4.Chronic Pain and High-impact Chronic Pain Among U.S. Adults, 2019 https://www.cdc.gov/nchs/products/databriefs/db390.htm Accessed: March 10, 2023
- 5.International Association for the Study of Pain. IASP Taxonomy. Revised 2020. www.iasp-pain.org/Taxonomy. Accessed: March 10, 2023
- 6.Meints SM, Edwards RR. Evaluating psychosocial contributions to chronic pain outcomes. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87(Pt B):168-182.
- 7.Rashid,H (2022)Physiology of pain pathways. Retrieved from https://www.slideshare.net/hassandoc90/physiology-of-pain-pathways
- 8.Kawai K, Kawai AT, Wollan P, Yawn BP. Adverse impacts of chronic pain on health-related quality of life, work productivity, depression and anxiety in a community-based study. Fam Pract. 2017;34(6):656-661.
- 9.Lewis, Melba J. Moreland MSN, CCRC; Kohtz, Cindy EdD, MSN, RN, CNE; Emmerling, Sheryl PhD, NEA-BC; Fisher, Mary MA, MSN, RN, NEA-BC; Mcgarvey, Jeremy MS Pain control and nonpharmacologic interventions, Nursing: September 2018 - Volume 48 - Issue 9 - p 65-68
- 10.Sullivan MJ, Neish N. The effects of disclosure on pain during dental hygiene treatment: the moderating role of catastrophizing. Pain. 1999;79(2-3):155-163. doi:10.1016/s0304-3959(98)00163-8.
- 11.Positioning for success.https://www.rdhmag.com/career-profession/students/article/16405973/positioning-for-success. January 1, 2012. Accessed: August 1, 2021
- 12.Brady, M.,Alvear,B, Meeting Patient’s Pain Management Needs, Special Edition- Dimensions of Dental Hygiene, March 2021;19(3):16, 18, 21.
- 13.Khera T, Rangasamy V. Cognition and Pain: A Review. Front Psychol. 2021;12:673962. Published 2021 May 21. doi:10.3389/fpsyg.2021.673962
- 14.Orhurhu VJ, Roberts JS, Ly N, et al. Ketamine In Acute and Chronic Pain Management. Updated : 2022 Sep 19. StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539824/
- 15.Doody O, Bailey ME. Understanding pain physiology and its application to person with intellectual disability. J Intellect Disabil. 2019;23(1):5-18. doi:10.1177/1744629517708680
- 16.Quinlan, Jane FRCA, FFPMRCA,; Cox, Felicia FRCN. Acute pain management in patients with drug dependence syndrome. PAIN Reports 2(4):p e611, July/August 2017.
- 17.Sheng J, Liu S, Wang Y, Cui R, Zhang X. The Link between Depression and Chronic Pain: Neural Mechanisms in the Brain. Neural Plast. 2017;2017:9724371. doi:10.1155/2017/9724371
- 18.Mills SEE, Nicolson KP, Smith BH. Chronic pain: a review of its epidemiology and associated factors in population-based studies. Br J Anaesth. 2019;123(2):e273-e283. doi:10.1016/j.bja.2019.03.023
- 20.Tan HL, Smith JG, Hoffmann J, Renton T. A systematic review of treatment for patients with burning mouth syndrome. Cephalalgia. 2022;42(2):128-161. doi:10.1177/03331024211036152
- 21.Brody, A., Novel Therapy May Relieve Temporomandibular Joint Pain, https://dimensionsofdentalhygiene.com/novel-therapy-may-relieve-temporomandibular-joint-pain/ Accessed: January 18, 2023.
- 22.Epstein JB, Miaskowski C. Oral Pain in the Cancer Patient. J Natl Cancer Inst Monogr. 2019;2019(53):lgz003. doi:10.1093/jncimonographs/lgz003
- 23.Riggs A, Breuer B, Patel V, et al. Pain-related distress among patients referred to a community-based palliative care program. Palliat Support Care. 2019;17(3):338-344.
- 24.Toyofuku A. Psychosomatic problems in dentistry. Biopsychosoc Med. 2016;10:14. Published 2016 Apr 30. doi:10.1186/s13030-016-0068-2
- 25.Schramm E, Waisman A. Microglia as Central Protagonists in the Chronic Stress Response. Neurol Neuroimmunol Neuroinflamm. 2022;9(6):e200023. Published 2022 Sep 7. doi:10.1212/NXI.0000000000200023
- 26.Geva N, Defrin R. Opposite Effects of Stress on Pain Modulation Depend on the Magnitude of Individual Stress Response. J Pain. 2018 Apr;19(4):360-371. doi:10.1016/j.jpain.2017.11.011
- 27.Abdallah CG, Geha P. Chronic Pain and Chronic Stress: Two Sides of the Same Coin?. Chronic Stress (Thousand Oaks). 2017;1:2470547017704763. doi:10.1177/2470547017704763
- 28.Sullivan MD, Ballantyne JC. Must we reduce pain intensity to treat chronic pain?. Pain. 2016;157(1):65-69. doi:10.1097/j.pain.0000000000000336
- 29.Sullivan MD, Ballantyne JC. When Physical and Social Pain Coexist: Insights Into Opioid Therapy. Ann Fam Med. 2021;19(1):79-82. doi:10.1370/afm.2591
- 30.Domenichiello AF, Ramsden CE. The silent epidemic of chronic pain in older adults. Prog Neuropsychopharmacol Biol Psychiatry. 2019 Jul 13; 93:284-290. doi:10.1016/j.pnpbp.2019.04.006
- 31.Geva N, Golan S, Pinchas L, Defrin R. Sex effects in the interaction of acute stress and pain perception. Pain. 2023;164(3):587-597. doi:10.1097/j.pain.0000000000002743
- 32.Keogh E. Sex and Gender Differences in Pain Across the Life Course. Handbook of Pain and Palliative Care 2018. Doi : 10.1007/978-3-319-95369-4_18
- 33.Hasenfratz K, Moergeli H, Sprott H, Ljutow A, Hefti R, Rittmayer I, Peng-Keller S and Rufer M (2021) Do Chronic Pain Patients Wish Spiritual Aspects to Be Integrated in Their Medical Treatment? A Cross-Sectional Study of Multiple Facilities. Front. Psychiatry 12:685158.
- 34.Sharma S, Abbott JH, Jensen MP. Why clinicians should consider the role of culture in chronic pain. Braz J Phys Ther. 2018;22(5):345-346.
- 35.Carteret,M. https://www.dimensionsofculture.com/2010/11/cultural-aspects-of-pain-management/ Accessed: April 1,2022
- 36.Simon, E., Zsidó, A.N., Birkás, B. et al. Pain catastrophizing, pain sensitivity and fear of pain are associated with early life environmental unpredictability: a path model approach. BMC Psychol 10, 97 (2022).
- 37.Köppen PJ, Dorner TE, Stein KV, Simon J, Crevenna R. Health literacy, pain intensity and pain perception in patients with chronic pain. Wien Klin Wochenschr. 2018 Jan;130(1-2):23-30. doi:10.1007/s00508-017-1309-5
- 38.Banozic A, Miljkovic A, Bras M, Puljak L, Kolcic I, Hayward C, Polasek O. Neuroticism and pain catastrophizing aggravate response to pain in healthy adults: an experimental study. Korean J Pain. 2018 Jan;31(1):16-26. doi:10.3344/kjp.2018.31.1.16
- 39.Castellanos, S., Dental Hygiene Approach Toward COVID-19, Dimensions of Dental Hygiene,February 2021, pgs.40-43.
- 40.Swann M. Recognising the importance of language in effective pain assessment. Nurs Stand. 2021;36(2):43-50. doi:10.7748/ns.2021.e11563
- 41.Timmerman A, Parashos P. Management of dental pain in primary care. Aust Prescr. 2020;43(2):39-44. doi:10.18773/austprescr.2020.010
- 42.Guidetti S, Nielsen KT, von Bülow C, Sampedro-Pilegaard M,Klokker, L,Waehrens,E E, Evaluation of an intervention programme addressing ability to perform activities of daily living among persons with chronic conditions: study protocol for a feasibility trial (ABLE) BMJ Open 2018;8:e020812. doi: 10.1136/bmjopen-2017-020812
- 43.Edemekong PF, Bomgaars DL, Sukumaran S, Schoo C. Activities of Daily Living. In: StatPearls. Treasure Island (FL): StatPearls Publishing; November 19, 2022.
- 44.Berggren K, Broström A, Firestone A, Wright B, Josefsson E, Lindmark U. Oral health problems linked to obstructive sleep apnea are not always recognized within dental care-As described by dental professionals. Clin Exp Dent Res. 2022;8(1):84-95.
- 45.Wachholtz A, Robinson D, Epstein E. Developing a novel treatment for patients with chronic pain and Opioid User Disorder. Subst Abuse Treat Prev Policy. 2022;17(1):35. Published 2022 May 7. doi:10.1186/s13011-022-00464-4
- 46.Singh, N.,Providing Care to Patients with Special Needs Dimensions of Dental Hygiene. July/August 2019;17(7):46–49. Accessed: March 1, 2023.
- 47.Shirley Musich, Shaohung S. Wang, Joann Ruiz, Kevin Hawkins, Ellen Wicker, The impact of mobility limitations on health outcomes among older adults, Geriatric Nursing, Volume 39, Issue 2, 2018, Pages 162-169,
- 48.Moore, T., Dental Care for Patients with Special Needs, Decisions in Dentistry. September 2016;2(09):50–53. Accessed: March 1, 2023.
- 49.Janto M, Iurcov R, Daina CM, Neculoiu DC, Venter AC, Badau D, Cotovanu A, Negrau M, Suteu CL, Sabau M, Daina LG. Oral Health among Elderly, Impact on Life Quality, Access of Elderly Patients to Oral Health Services and Methods to Improve Oral Health: A Narrative Review. Journal of Personalized Medicine. 2022; 12(3):372.
- 50.Freiwald J, Magni A, Fanlo-Mazas P, Paulino E, Sequeira de Medeiros L, Moretti B, Schleip R, Solarino G. A Role for Superficial Heat Therapy in the Management of Non-Specific, Mild-to-Moderate Low Back Pain in Current Clinical Practice: A Narrative Review. Life. 2021.
- 51.D’Arro, C. (2018). Mindful Dentist. The International Journal of Whole Person Care, 5(2). https://doi.org/10.26443/ijwpc.v5i2.182
- 52.Xu, Jianghan BS; Wu, Boyi BS; Xie, Shengji BS; Wu, Guanghui BS; Zhang, Heng BS; Fu, Yangyang MM; Guo, Guangxin MD,. Effectiveness and safety of massage for chronic pain in patients with knee osteoarthritis: A protocol for systematic review and meta-analysis. Medicine 101(3):p e28533, January 21, 2022.
- 53.Xiang A, Cheng K, Shen X, Xu P, Liu S. The Immediate Analgesic Effect of Acupuncture for Pain: A Systematic Review and Meta-Analysis. Evid Based Complement Alternat Med. 2017;2017:3837194. doi:10.1155/2017/3837194
- 54.Lim JA, Choi SH, Lee WJ, et al. Cognitive-behavioral therapy for patients with chronic pain: Implications of gender differences in empathy. Medicine (Baltimore). 2018;97(23):e10867. doi:10.1097/MD.0000000000010867
- 55.Vambheim SM, Kyllo TM, Hegland S, Bystad M. Relaxation techniques as an intervention for chronic pain: A systematic review of randomized controlled trials. Heliyon. 2021;7(8):e07837. Published 2021 Aug 20. doi:10.1016/j.heliyon.2021.e07837
- 56.Cho MK, Choi MY. Effect of Distraction Intervention for Needle-Related Pain and Distress in Children: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2021;18(17):9159. Published 2021 Aug 31. doi:10.3390/ijerph18179159
- 57.Wieland LS, Skoetz N, Pilkington K, Harbin S, Vempati R, Berman BM. Yoga for chronic non-specific low back pain. Cochrane Database Syst Rev. 2022;11(11):CD010671. Published 2022 Nov 18.
- 58.Whitlock EL, Diaz-Ramirez LG, Glymour MM, Boscardin WJ, Covinsky KE, Smith AK. Association Between Persistent Pain and Memory Decline and Dementia in a Longitudinal Cohort of Elders. JAMA Intern Med. 2017 Aug 1;177(8):1146-1153