:sharpen(level=0):output(format=jpeg)/up/2023/05/Fiona-Collins-thumbnail-1-3.jpg "Fiona Collins")
:sharpen(level=0):output(format=jpeg)/up/2022/05/psoriasis_psoriatic_arthitis-2.jpg "Only Skin Deep? Psoriasis, Psoriatic Arthritis and Periodontitis")
Only Skin Deep? Psoriasis, Psoriatic Arthritis and Periodontitis
Periodontitis (CP) is a multifactorial chronic inflammatory disease that has a strong bidirectional relationship with diabetes mellitus, associations with cardiovascular disease and Alzheimer’s disease, and links to other systemic diseases.1Sanz M, Ceriello A, Buysschaert M et al. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International Diabetes Federation and the European Federation of Periodontology. J Clin Periodontol 2018;45(2):138-49. doi: 10.1111/jcpe.12808. ,2Genco RJ, Sanz M. Clinical and public health implications of periodontal and systemic diseases: An overview. Periodontol 2000 2020;83(1):7-13. doi: 10.1111/prd.12344. In addition, several systemic chronic inflammatory conditions and CP frequently co-exist in individuals, with higher levels of inflammatory responses than the general population.3Bunte K, Beikler T. Th17 Cells and the IL-23/IL-17 Axis in the Pathogenesis of Periodontitis and Immune-Mediated Inflammatory Diseases. Int J Mol Sci2019;20(14):3394. doi: 10.3390/ijms20143394. A significant amount of research now also exists for a relationship between CP and rheumatoid arthritis.4González-Febles J, Sanz M. Periodontitis and rheumatoid arthritis: What have we learned about their connection and their treatment? Periodontol 2000 2021;87(1):181-203. doi: 10.1111/prd.12385. Emerging science suggests a potential association for psoriasis (Ps), psoriatic arthritis (PsA) and CP, which are the most frequently occurring chronic inflammatory diseases.5Mendes VS, Cota LOM, Costa AA et al. Periodontitis as another comorbidity associated with psoriasis: A case-control study. J Periodontol 2019;90(4):358-66. doi: 10.1002/JPER.18-0394.,6Sezer U, Şenyurt SZ, Gündoğar H et al. Effect of Chronic Periodontitis on Oxidative Status in Patients With Psoriasis and Psoriatic Arthritis. J Periodontol 2016;87(5):557-65. doi: 10.1902/jop.2015.150337. In this article we will review available information on psoriatic disease and its potential association with CP.
Figure 1. Healthy skin and psoriatic lesions

Source: Jacky Co/ Shutterstock
Ps and PsA
Ps is a chronic autoimmune disorder involving a dysregulated immune response, with a prevalence of around 3% globally.7Üstün K, Sezer U, Kısacık B et al. Periodontal disease in patients with psoriatic arthritis. Inflammation 2013;36(3):665-9. doi: 10.1007/s10753-012-9590-y.,8Crincoli V, Di Comite M, Di Bisceglie MB et al. Temporomandibular Disorders in Psoriasis Patients with and without Psoriatic Arthritis: An Observational Study. Int J Med Sci 2015;12(4):341-8. doi:10.7150/ijms.11288,9Liang Y, Sarkar MK, Tsoi LC, Gudjonsson JE. Psoriasis: a mixed autoimmune and autoinflammatory disease. Curr Opin Immunol 2017;49:1-8.,10Yan D, Gudjonsson JE, Le S et al. New Frontiers in Psoriatic Disease Research, Part I: Genetics, Environmental Triggers, Immunology, Pathophysiology, and Precision Medicine. J Invest Dermatol 2021;141(9):2112-22.e3. doi: 10.1016/j.jid.2021.02.764. Ps can involve the skin (including the scalp), nails, and mucous membranes, and includes subtypes. In skin, an inflammatory process causes the production of excessive levels of keratinocytes which results in thickened plaque-like irritated areas. (Figure 1) This presentation is also referred to as plaque Ps. However, subtype inverse Psoriasis presents as a red, shiny, smooth rash in skin folds. Abnormal papillary capillaries and neovascularization also occur at the site of Ps lesions, as well as intraepidermal neutrophil micro-abscess.9Liang Y, Sarkar MK, Tsoi LC, Gudjonsson JE. Psoriasis: a mixed autoimmune and autoinflammatory disease. Curr Opin Immunol 2017;49:1-8. Psoriatic inflammation exhibits periods of exacerbation and remission. Risk factors include a strong genetic component and environmental triggers including emotional stress, alcohol consumption, medications, skin trauma, infections, biomechanical stress, obesity, and endocrine disorders.10Yan D, Gudjonsson JE, Le S et al. New Frontiers in Psoriatic Disease Research, Part I: Genetics, Environmental Triggers, Immunology, Pathophysiology, and Precision Medicine. J Invest Dermatol 2021;141(9):2112-22.e3. doi: 10.1016/j.jid.2021.02.764.,11Gonzaga HF, Chaves MD, Gonzaga LH et al. Environmental factors in benign migratory glossitis and psoriasis: retrospective study of the association of emotional stress and alcohol and tobacco consumption with benign migratory glossitis and cutaneous psoriasis. J Eur Acad Dermatol Venereol 2015;29(3):533-6. doi: 10.1111/jdv.12616. (Table 1)
Patients with Ps can also develop PsA. The prevalence of PsA in patients with Ps is around 30%, with a range from 5% to 70% cited in the literature.5Mendes VS, Cota LOM, Costa AA et al. Periodontitis as another comorbidity associated with psoriasis: A case-control study. J Periodontol 2019;90(4):358-66. doi: 10.1002/JPER.18-0394.,9Liang Y, Sarkar MK, Tsoi LC, Gudjonsson JE. Psoriasis: a mixed autoimmune and autoinflammatory disease. Curr Opin Immunol 2017;49:1-8.,12Badel T, Savić Pavičin I, Krapac L et al. Psoriatic arthritis and temporomandibular joint involvement – literature review with a reported case. Acta Dermatovenerol Croat 2014;22(2):114-21. PsA is a chronic seronegative arthritis, usually preceded by psoriasis, and results in progressive inflammatory joint damage.7Üstün K, Sezer U, Kısacık B et al. Periodontal disease in patients with psoriatic arthritis. Inflammation 2013;36(3):665-9. doi: 10.1007/s10753-012-9590-y.,13Sakkas LI, Bogdanos DP. Are psoriasis and psoriatic arthritis the same disease? The IL-23/IL-17 axis data. Autoimmun Rev 2017;16(1):10-5. doi: 10.1016/j.autrev.2016.09.015.
| Table 1. Risk Factors for Ps |
|---|
| Genetics |
| Emotional stress |
| Alcohol consumption |
| Obesity |
| Endocrine disorders |
| Medications |
| Skin Trauma |
| Biomechanical stress |
| Infections |
| Smoking |
Figure 2. Basics of the inflammatory cascade in Ps
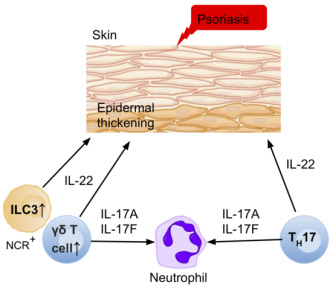
Source: Mk4716. ILCs involved in the pathophysiology of psoriasis.
https://commons.wikimedia.org/wiki/File:ILCs_in_psoriasis_10_PNG.png
The Inflammatory Cascade
The development and progression of Ps results from an immune-driven inflammatory cascade involving cytokines and chemokines. The T helper 17 cell population (Th17), a subset of CD4 T cells, is maintained and increased by IL-23.14Malakouti M, Brown GE, Wang E et al. The role of IL-17 in psoriasis. J Dermatolog Treat 2015;26(1):41-4. doi: 10.3109/09546634.2013.879093. Th17 secrete IL-17 and IL-22. The IL-23/IL-17 pathway is considered to have a key role in the development and progression of both PsA and Ps as well as other autoimmune conditions.13Sakkas LI, Bogdanos DP. Are psoriasis and psoriatic arthritis the same disease? The IL-23/IL-17 axis data. Autoimmun Rev 2017;16(1):10-5. doi: 10.1016/j.autrev.2016.09.015.,14Malakouti M, Brown GE, Wang E et al. The role of IL-17 in psoriasis. J Dermatolog Treat 2015;26(1):41-4. doi: 10.3109/09546634.2013.879093. While IL-17F is protective against infections, IL-17A mediates the innate immune response but also acts as a pro-inflammatory cytokine.15Zenobia C, Hajishengallis G. Basic biology and role of interleukin-17 in immunity and inflammation. Periodontology 2000 2015;69:142-59. doi 10.1111/prd.12083.,16Feng Y, Chen Z, Tu SQ et al. Role of Interleukin-17A in the Pathomechanisms of Periodontitis and Related Systemic Chronic Inflammatory Diseases. Front Immunol 2022;13:862415. doi: 10.3389/fimmu.2022.862415. IL-17A in turn promotes production of IL-1, IL-6, TNF-alpha and other pro-inflammatory factors. Overexpression of TNF-alpha causes rapid proliferation of keratinocytes (Ps) and bony destruction (PsA). Pro-inflammatory mediators such as matrix metalloproteinases (MMPs), RANKL and VEGF also result in tissue destruction. IL-12, IL-17, IL-22, and IL-23 are all involved in psoriatic inflammation.17National Psoriasis Foundation. Drugs that are associated with dry mouth. https://www.ehealthme.com/side-effect/dry-mouth/t/1/. Furthermore, higher levels of IL-22 are found in skin lesions (Ps) and connective tissues than in joints, and IL-22 promotes bone formation, while high levels of IL-17 have been found for PsA and Ps. 13Sakkas LI, Bogdanos DP. Are psoriasis and psoriatic arthritis the same disease? The IL-23/IL-17 axis data. Autoimmun Rev 2017;16(1):10-5. doi: 10.1016/j.autrev.2016.09.015.,14Malakouti M, Brown GE, Wang E et al. The role of IL-17 in psoriasis. J Dermatolog Treat 2015;26(1):41-4. doi: 10.3109/09546634.2013.879093. (Figure 2)
The inflammatory cascade associated with Th17 and IL-17/IL-23 is also involved in the development and progression of other systemic immune-related conditions as well as CP.3Bunte K, Beikler T. Th17 Cells and the IL-23/IL-17 Axis in the Pathogenesis of Periodontitis and Immune-Mediated Inflammatory Diseases. Int J Mol Sci2019;20(14):3394. doi: 10.3390/ijms20143394.,18Beklen A, Ainola M, Hukkanen M et al. MMPs, IL-1, and TNF are Regulated by IL-17 in Periodontitis. J Dent Res 2007;86(4):347-51. doi:0.1177/154405910708600409. In addition, in recent research, higher levels of IL-17A, IL-22 and IL-23 have been found in the gingival crevicular fluid of patients with Ps and moderate/severe CP compared to individuals with mild CP or who are periodontally healthy.19Jiménez C, Carvajal D, Hernández M et al. Levels of the Interleukins 17A, 22, and 23 and the S100 Protein Family in the Gingival Crevicular Fluid of Psoriatic Patients With or Without Periodontitis. Bras Dermatol 2021;96(2):163-70. doi: 10.1016/ j.abd.2020.08.008 In other research, higher concentrations of oral bacterial DNA were found in synovial fluid in patients with PsA (and patients with RA) than in other individuals.20Moen K, Brun JG, Valen M et al. Synovial inflammation in active rheumatoid arthritis and psoriatic arthritis facilitates trapping of a variety of oral bacterial DNAs. Clin Exp Rheumatol 2006;24(6):656-63. Porphyromonas gingivalis and Prevotella nigrescens were only found in the synovial fluids of patients with PsA or RA.
Studies on CP and Ps/PsA
Researchers have studied the potential influence of Ps and PsA on CP, and the potential influence of CP on Ps and PsA.
CP in individuals with Ps, PsA
In a quantitative meta-analysis of 8 studies conducted between 2013 and 2019, individuals with Ps were found to have poorer periodontal health and greater clinical attachment loss than individual without Ps.21Qiao P, Shi Q, Zhang R et al. Psoriasis Patients Suffer From Worse Periodontal Status-A Meta-Analysis. Front Med (Lausanne) 2019;6:212. doi: 10.3389/fmed.2019.00212. However, most studies were case control studies with varying study methodologies, weakening these findings. In a nationwide cohort study in Denmark, 5 million individuals at least 18 years-of-age between 1997 and 2011 were included.22Egeberg A, Mallbris L, Gislason G et al. Risk of periodontitis in patients with psoriasis and psoriatic arthritis. J Eur Acad Dermatol Venereol 2017;31(2):288-93. doi: 10.1111/jdv.13814. Risk for CP increased by more than half, double and triple, respectively, for individuals with mild Ps, severe Ps and PsA. In a nationwide retrospective cohort study in Taiwan, subjects included individuals diagnosed with psoriatic disease between 2003 and 2011 and individuals without Ps.23Su NY, Huang JY, Hu CJ et al. Increased risk of periodontitis in patients with psoriatic disease: a nationwide population-based retrospective cohort study. Peer J. 2017;5:e4064. doi: 10.7717/peerj.4064. A greater risk of developing CP and more severe CP was found for the group with PsA compared to individuals with or without Ps.
In a prospective case control study with 201 patients, individuals with Ps had greater periodontal inflammation.24Woeste S, Graetz C, Gerdes S, Mrowietz U. Oral Health in Patients with Psoriasis-A Prospective Study. J Invest Dermatol 2019;139(6):1237-44. doi: 10.1016/j.jid.2018.12.014. In another case control study, a higher prevalence of CP was found for patients with moderate/severe Ps compared to the control group.25Skudutyte-Rysstad R, Slevolden EM, Hansen BF et al. Association between moderate to severe psoriasis and periodontitis in a Scandinavian population. BMC Oral Health 2014;14:139. doi 10.1186/1472-6831-14-139. A 72% greater risk for CP was found for individuals with Ps in a recent case-control study with more than seven hundred individuals, and a greater prevalence of CP for more severe Ps.5Mendes VS, Cota LOM, Costa AA et al. Periodontitis as another comorbidity associated with psoriasis: A case-control study. J Periodontol 2019;90(4):358-66. doi: 10.1002/JPER.18-0394. In one study, researchers found a more than five-fold risk for CP for the group with inverse type Ps compared to the group with typical Ps.26Painsi C, Hirtenfelder A, Lange-Asschenfeldt B et al. The Prevalence of Periodontitis Is Increased in Psoriasis and Linked to Its Inverse Subtype. Skin Pharmacol Physiol 2017;30(6):324-8. doi: 10.1159/000481544. A higher prevalence of CP and more severe CP has also been found for patients with PsA compared to those without PsA.7Üstün K, Sezer U, Kısacık B et al. Periodontal disease in patients with psoriatic arthritis. Inflammation 2013;36(3):665-9. doi: 10.1007/s10753-012-9590-y.,27Mishra S, Johnson L, Agrawal S, Rajput S. Assessment of Periodontal status in Patients with Psoriatic Arthritis: A retrospective, case-control study. J Clin Exp Dent 2021;13(8):e776-83. Conversely, one study found no increase in risk for CP in relation to the presence of Ps.28Fadel HT, Flytström I, Calander AM et al. Profiles of dental caries and periodontal disease in individuals with or without psoriasis. J Periodontol 2013;84(4):477-85. doi: 10.1902/jop.2012.120119. In a second study measuring antioxidant levels in patients with and without PS or PsA and with or without CP, clinical parameters were unaffected by Ps or PsA.6Sezer U, Şenyurt SZ, Gündoğar H et al. Effect of Chronic Periodontitis on Oxidative Status in Patients With Psoriasis and Psoriatic Arthritis. J Periodontol 2016;87(5):557-65. doi: 10.1902/jop.2015.150337.
Ps, PsA in individuals with CP
In a prospective cohort study with more than 60,000 nurses, risk for Ps in individuals with CP was evaluated.29Nakib S, Han J, Li T et al. Periodontal disease and risk of psoriasis among nurses in the United States. Acta Odontol Scand 2013;71:1423-9. doi: 10.3109/00016357.2013.766360. After adjusting for confounders (age, physical activity, tooth loss, body mass index, cigarette smoking and alcohol consumption), risk for developing Ps increased by 35% and 49% for individuals with mild and moderate/severe CP, respectively. One study limitation was that CP (bone loss) was self-reported. In a second cohort study with more than 230,000 individuals, at 5 years the risk of developing Ps was 52% higher for individuals with CP compared to the periodontally healthy group.30Keller JJ, Lin HC. The effects of chronic periodontitis and its treatment on the subsequent risk of psoriasis. Brit J Dermatol 2012;167:1338-44. Doi 10.1111/j.1365-2133.2012.11126.x. In a meta-analysis conducted to evaluate the potential association between Ps and CP, an almost three-fold risk for Ps was found for individuals with CP.31Zhang X, Gu H, Xie S, Su Y. Periodontitis in patients with psoriasis: A systematic review and meta-analysis. Oral Dis 2022;28(1):33-43. doi: 10.1111/odi.13617. However, studies used differing methodologies, did not all consider confounders, and seven of the 9 studies included were case controlled, weakening the findings. In a case control study conducted in 2013, Ps and CP were significantly correlated.32Lazaridou E, Tsikrikoni A, Fotiadou C et al. Association of chronic plaque psoriasis and severe periodontitis: a hospital based case-control study. J Eur Acad Dermatol Venereol 2013;27:967-72 doi 10.1111/j.1468-3083.2012.04615.x.
Effect of periodontal therapy
There is limited data on the effect of periodontal therapy on Ps and PsA. In a randomized controlled trial with subjects with CP and Ps, non-surgical periodontal therapy resulted in lower levels of IL-2 and IL-6 and less severe Ps eight weeks post-treatment compared to levels found for the control group awaiting periodontal therapy.33Ucan Yarkac F, Ogrum A, Gokturk O. Effects of non-surgical periodontal therapy on inflammatory markers of psoriasis: A randomized controlled trial. J Clin Periodontol 2020;47(2):193-201. doi: 10.1111/jcpe.13205. In one study, periodontal therapy reduced risk for future Ps.30Keller JJ, Lin HC. The effects of chronic periodontitis and its treatment on the subsequent risk of psoriasis. Brit J Dermatol 2012;167:1338-44. Doi 10.1111/j.1365-2133.2012.11126.x.
Oral manifestations of Ps and PsA
Figure 3. Geographic tongue
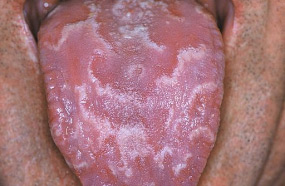
Source: D Malamos.
https://commons.wikimedia.org/wiki/File:Geographic_tongue_01.JPG
Oral manifestations reported are primarily geographic tongue (GT). (Figure 3) In a review of eleven case control studies, a three-fold prevalence of GT was found for patients with Ps compared to the control group.34González-Álvarez L, García-Martín JM, García-Pola MJ. Association between geographic tongue and psoriasis: A systematic review and meta-analyses. J Oral Pathol Med 2019;48(5):365-72. doi: 10.1111/jop.12840. In addition, individuals with GT exhibited more severe Ps in 3 of the 4 studies assessing this variable. In a recent case control study, more than three times as many oral lesions were seen in the Ps group than in the control group, specifically GT and angular cheilitis.35Costa AA, Cota LOM, Mendes VS et al. Impact of oral lesions on the quality of life of psoriatic individuals: A case-control study. Oral Dis 2021;27(7):1813-21. doi: 10.1111/odi.13695. Other studies report an increased prevalence of GT and fissured tongue in patients with Ps.36Picciani B, Santos T, Domingos C et al. Geographic tongue and fissured tongue in 348 patients with psoriasis: correlation with disease severity. Sci World J 2015;2015:564326.,37Germi L, De Giorgi V, Bergamo F et al. Psoriasis and oral lesions: multicentric study of Oral Mucosa Diseases Italian Group (GIPMO). Dermatol Online J 2012:18(1): 11. ,38Talaee R, Hajheydari Z, Moghaddam AY et al. Prevalence of Oral Mucosal Lesions and Their Association with Severity of Psoriasis among Psoriatic Patients Referred To Dermatology Clinic: A Cross-Sectional Study in Kashan/Iran. Open Access Maced J Med Sci 2017;5(7):978-82. doi: 10.3889/oamjms.2017.189.,39Monson CA, Silva V, Porfírio G et al. Oral Health Issues in Psoriasis: An Overview of the Literature. Int J Clin Dermatol & Res 2016;94-103. Doi: 10.19070/2332-2977-1600025.,40Olejnik M, Osmola-Mańkowska A, Ślebioda Z et al. Oral mucosal lesions in psoriatic patients based on disease severity and treatment approach. J Oral Pathol Med 2020;49(8):822-8. doi: 10.1111/jop.13095. Two studies resulted in the conclusion that GT may be a biomarker for Ps severity,36Picciani B, Santos T, Domingos C et al. Geographic tongue and fissured tongue in 348 patients with psoriasis: correlation with disease severity. Sci World J 2015;2015:564326.,41Zargari O. The prevalence and significance of fissured tongue and geographical tongue in psoriatic patients. Clin and Exper Dermatol 2006;31(2):192-5. doi: 10.1111/j.1365-2230.2005.02028.x. while in another study no such relationship was found.40Olejnik M, Osmola-Mańkowska A, Ślebioda Z et al. Oral mucosal lesions in psoriatic patients based on disease severity and treatment approach. J Oral Pathol Med 2020;49(8):822-8. doi: 10.1111/jop.13095. More severe GT has been found in patients with Ps, and it was proposed that GT in these patients is oral psoriasis.42Picciani B, Santos VC, Teixeira-Souza T et al. Investigation of the clinical features of geographic tongue: unveiling its relationship with oral psoriasis. Int J Dermatol 2017;56(4):421-7. doi: 10.1111/ijd.13460. GT is a chronic, inflammatory and ‘immune-mediated’ condition, with an inflammatory process similar to Ps, including the role of Th17, IL-17 and IL-23.43Picciani BLS, Domingos TA, Teixeira-Souza T et al. Evaluation of the Th17 pathway in psoriasis and geographic tongue. An Bras Dermatol 2019;94(6):677-83. doi: 10.1016/j.abd.2019.01.006.
Researchers have found a significant increase in signs and symptoms of TMD (bruxism, limited opening, clicking sounds and orofacial pain) in patients with Ps, and more so in patients with PSA.8Crincoli V, Di Comite M, Di Bisceglie MB et al. Temporomandibular Disorders in Psoriasis Patients with and without Psoriatic Arthritis: An Observational Study. Int J Med Sci 2015;12(4):341-8. doi:10.7150/ijms.11288,39Monson CA, Silva V, Porfírio G et al. Oral Health Issues in Psoriasis: An Overview of the Literature. Int J Clin Dermatol & Res 2016;94-103. Doi: 10.19070/2332-2977-1600025. Typical signs of PsA are found during magnetic resonance imaging, including bony erosions and articular effusion.12Badel T, Savić Pavičin I, Krapac L et al. Psoriatic arthritis and temporomandibular joint involvement – literature review with a reported case. Acta Dermatovenerol Croat 2014;22(2):114-21.
| Table 2. Oral manifestations reported for Ps and PsA |
|---|
| Geographic tongue |
| Fissured tongue |
| Angular cheilitis |
| TMJ disorder |
| Other oral lesions |
Other Considerations
Medications used to treat psoriatic disease include hydrocortisone, non-steroidal anti-inflammatories, methotrexate (an anti-neoplastic drug), cyclosporine (an immunosuppressant), retinoids (acitracin, Soriatane), and biologics.39Monson CA, Silva V, Porfírio G et al. Oral Health Issues in Psoriasis: An Overview of the Literature. Int J Clin Dermatol & Res 2016;94-103. Doi: 10.19070/2332-2977-1600025.,44National Psoriasis Foundation. Soriatane (Acitretin). https://www.psoriasis.org/soriatane-acitretin/. Biologics currently used to treat psoriatic disease are delivered by injection.39Monson CA, Silva V, Porfírio G et al. Oral Health Issues in Psoriasis: An Overview of the Literature. Int J Clin Dermatol & Res 2016;94-103. Doi: 10.19070/2332-2977-1600025.,45National Psoriasis Foundation. Current Biologics on the Market. https://www.psoriasis.org/current-biologics-on-the-market/. These include IL-17 inhibitors (Cosentyx, secukinumab; Siliq, brodalumab; Taltz, ixekizumab), an IL-12 and Il-23 inhibitor (Stelara, ustekinumab), IL-23 inhibitors (Ilumya, tildrakizumab-asmn; Skyrizi, risankizumab-rzaa; Tremfya, guselkumab), TNF-alpha inhibitors such as Enbrel (etanercept) and Humira (adalimumab), and a T-cell inhibitor (Orencia, abatacept).
The medication used depends on the type and severity of psoriatic disease. Oral adverse events may also occur.39Monson CA, Silva V, Porfírio G et al. Oral Health Issues in Psoriasis: An Overview of the Literature. Int J Clin Dermatol & Res 2016;94-103. Doi: 10.19070/2332-2977-1600025. Retinoids can cause dry mouth and gingival bleeding, cyclosporine can cause gingival hyperplasia, reports of mucositis have occurred with methotrexate use, and there have been reports of dry mouth for some biologics.18Beklen A, Ainola M, Hukkanen M et al. MMPs, IL-1, and TNF are Regulated by IL-17 in Periodontitis. J Dent Res 2007;86(4):347-51. doi:0.1177/154405910708600409. Drug contraindications and systemic adverse events are outwith the scope of this article.
Conclusions
CP and Ps/PsA are multifactorial chronic diseases with inflammatory cascades involving IL-17 and with other chemokines and cytokines in common. Risk factors also overlap. CP may play a role in the development or increased severity of Ps and it may also negatively impact the effectiveness of treatment for Ps.46Dalmády S, Kemény L, Antal M, Gyulai R. Periodontitis: a newly identified comorbidity in psoriasis and psoriatic arthritis. Expert Rev Clin Immunol 2020;16(1):101-8. doi: 10.1080/1744666X.2019.1700113. However, neither causality nor a strong association have yet been determined. Researchers have noted study weaknesses, including methodologies and heterogeneity. Well-designed prospective studies have been recommended to determine the relationship between CP and Ps/PsA.16Feng Y, Chen Z, Tu SQ et al. Role of Interleukin-17A in the Pathomechanisms of Periodontitis and Related Systemic Chronic Inflammatory Diseases. Front Immunol 2022;13:862415. doi: 10.3389/fimmu.2022.862415.,21Qiao P, Shi Q, Zhang R et al. Psoriasis Patients Suffer From Worse Periodontal Status-A Meta-Analysis. Front Med (Lausanne) 2019;6:212. doi: 10.3389/fmed.2019.00212.,31Zhang X, Gu H, Xie S, Su Y. Periodontitis in patients with psoriasis: A systematic review and meta-analysis. Oral Dis 2022;28(1):33-43. doi: 10.1111/odi.13617. Further research is also needed on the impact of non-surgical periodontal therapy on existing Ps/PsA, as well as potential improvement in CP with use of biologics to treat Ps and PsA.
In the meantime, patients with Ps/PsA should receive regular dental check-ups, including periodontal evaluations.23Su NY, Huang JY, Hu CJ et al. Increased risk of periodontitis in patients with psoriatic disease: a nationwide population-based retrospective cohort study. Peer J. 2017;5:e4064. doi: 10.7717/peerj.4064.,24Woeste S, Graetz C, Gerdes S, Mrowietz U. Oral Health in Patients with Psoriasis-A Prospective Study. J Invest Dermatol 2019;139(6):1237-44. doi: 10.1016/j.jid.2018.12.014.,46Dalmády S, Kemény L, Antal M, Gyulai R. Periodontitis: a newly identified comorbidity in psoriasis and psoriatic arthritis. Expert Rev Clin Immunol 2020;16(1):101-8. doi: 10.1080/1744666X.2019.1700113. Awareness of potential oral adverse events of Ps/PsA medication, preventive care for patients who may be experiencing dry mouth and treatment for other adverse events are important for oral health and quality of life. Dental professionals can help patients with Ps/PsA by educating them on the importance of preventing CP, the need to treat existing CP and to maintain oral health.
References
- 1.Sanz M, Ceriello A, Buysschaert M et al. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International Diabetes Federation and the European Federation of Periodontology. J Clin Periodontol 2018;45(2):138-49. doi: 10.1111/jcpe.12808.
- 2.Genco RJ, Sanz M. Clinical and public health implications of periodontal and systemic diseases: An overview. Periodontol 2000 2020;83(1):7-13. doi: 10.1111/prd.12344.
- 3.Bunte K, Beikler T. Th17 Cells and the IL-23/IL-17 Axis in the Pathogenesis of Periodontitis and Immune-Mediated Inflammatory Diseases. Int J Mol Sci2019;20(14):3394. doi: 10.3390/ijms20143394.
- 4.González-Febles J, Sanz M. Periodontitis and rheumatoid arthritis: What have we learned about their connection and their treatment? Periodontol 2000 2021;87(1):181-203. doi: 10.1111/prd.12385.
- 5.Mendes VS, Cota LOM, Costa AA et al. Periodontitis as another comorbidity associated with psoriasis: A case-control study. J Periodontol 2019;90(4):358-66. doi: 10.1002/JPER.18-0394.
- 6.Sezer U, Şenyurt SZ, Gündoğar H et al. Effect of Chronic Periodontitis on Oxidative Status in Patients With Psoriasis and Psoriatic Arthritis. J Periodontol 2016;87(5):557-65. doi: 10.1902/jop.2015.150337.
- 7.Üstün K, Sezer U, Kısacık B et al. Periodontal disease in patients with psoriatic arthritis. Inflammation 2013;36(3):665-9. doi: 10.1007/s10753-012-9590-y.
- 8.Crincoli V, Di Comite M, Di Bisceglie MB et al. Temporomandibular Disorders in Psoriasis Patients with and without Psoriatic Arthritis: An Observational Study. Int J Med Sci 2015;12(4):341-8. doi:10.7150/ijms.11288
- 9.Liang Y, Sarkar MK, Tsoi LC, Gudjonsson JE. Psoriasis: a mixed autoimmune and autoinflammatory disease. Curr Opin Immunol 2017;49:1-8.
- 10.Yan D, Gudjonsson JE, Le S et al. New Frontiers in Psoriatic Disease Research, Part I: Genetics, Environmental Triggers, Immunology, Pathophysiology, and Precision Medicine. J Invest Dermatol 2021;141(9):2112-22.e3. doi: 10.1016/j.jid.2021.02.764.
- 11.Gonzaga HF, Chaves MD, Gonzaga LH et al. Environmental factors in benign migratory glossitis and psoriasis: retrospective study of the association of emotional stress and alcohol and tobacco consumption with benign migratory glossitis and cutaneous psoriasis. J Eur Acad Dermatol Venereol 2015;29(3):533-6. doi: 10.1111/jdv.12616.
- 12.Badel T, Savić Pavičin I, Krapac L et al. Psoriatic arthritis and temporomandibular joint involvement – literature review with a reported case. Acta Dermatovenerol Croat 2014;22(2):114-21.
- 13.Sakkas LI, Bogdanos DP. Are psoriasis and psoriatic arthritis the same disease? The IL-23/IL-17 axis data. Autoimmun Rev 2017;16(1):10-5. doi: 10.1016/j.autrev.2016.09.015.
- 14.Malakouti M, Brown GE, Wang E et al. The role of IL-17 in psoriasis. J Dermatolog Treat 2015;26(1):41-4. doi: 10.3109/09546634.2013.879093.
- 15.Zenobia C, Hajishengallis G. Basic biology and role of interleukin-17 in immunity and inflammation. Periodontology 2000 2015;69:142-59. doi 10.1111/prd.12083.
- 16.Feng Y, Chen Z, Tu SQ et al. Role of Interleukin-17A in the Pathomechanisms of Periodontitis and Related Systemic Chronic Inflammatory Diseases. Front Immunol 2022;13:862415. doi: 10.3389/fimmu.2022.862415.
- 17.National Psoriasis Foundation. Drugs that are associated with dry mouth. https://www.ehealthme.com/side-effect/dry-mouth/t/1/.
- 18.Beklen A, Ainola M, Hukkanen M et al. MMPs, IL-1, and TNF are Regulated by IL-17 in Periodontitis. J Dent Res 2007;86(4):347-51. doi:0.1177/154405910708600409.
- 19.Jiménez C, Carvajal D, Hernández M et al. Levels of the Interleukins 17A, 22, and 23 and the S100 Protein Family in the Gingival Crevicular Fluid of Psoriatic Patients With or Without Periodontitis. Bras Dermatol 2021;96(2):163-70. doi: 10.1016/ j.abd.2020.08.008
- 20.Moen K, Brun JG, Valen M et al. Synovial inflammation in active rheumatoid arthritis and psoriatic arthritis facilitates trapping of a variety of oral bacterial DNAs. Clin Exp Rheumatol 2006;24(6):656-63.
- 21.Qiao P, Shi Q, Zhang R et al. Psoriasis Patients Suffer From Worse Periodontal Status-A Meta-Analysis. Front Med (Lausanne) 2019;6:212. doi: 10.3389/fmed.2019.00212.
- 22.Egeberg A, Mallbris L, Gislason G et al. Risk of periodontitis in patients with psoriasis and psoriatic arthritis. J Eur Acad Dermatol Venereol 2017;31(2):288-93. doi: 10.1111/jdv.13814.
- 23.Su NY, Huang JY, Hu CJ et al. Increased risk of periodontitis in patients with psoriatic disease: a nationwide population-based retrospective cohort study. Peer J. 2017;5:e4064. doi: 10.7717/peerj.4064.
- 24.Woeste S, Graetz C, Gerdes S, Mrowietz U. Oral Health in Patients with Psoriasis-A Prospective Study. J Invest Dermatol 2019;139(6):1237-44. doi: 10.1016/j.jid.2018.12.014.
- 25.Skudutyte-Rysstad R, Slevolden EM, Hansen BF et al. Association between moderate to severe psoriasis and periodontitis in a Scandinavian population. BMC Oral Health 2014;14:139. doi 10.1186/1472-6831-14-139.
- 26.Painsi C, Hirtenfelder A, Lange-Asschenfeldt B et al. The Prevalence of Periodontitis Is Increased in Psoriasis and Linked to Its Inverse Subtype. Skin Pharmacol Physiol 2017;30(6):324-8. doi: 10.1159/000481544.
- 27.Mishra S, Johnson L, Agrawal S, Rajput S. Assessment of Periodontal status in Patients with Psoriatic Arthritis: A retrospective, case-control study. J Clin Exp Dent 2021;13(8):e776-83.
- 28.Fadel HT, Flytström I, Calander AM et al. Profiles of dental caries and periodontal disease in individuals with or without psoriasis. J Periodontol 2013;84(4):477-85. doi: 10.1902/jop.2012.120119.
- 29.Nakib S, Han J, Li T et al. Periodontal disease and risk of psoriasis among nurses in the United States. Acta Odontol Scand 2013;71:1423-9. doi: 10.3109/00016357.2013.766360.
- 30.Keller JJ, Lin HC. The effects of chronic periodontitis and its treatment on the subsequent risk of psoriasis. Brit J Dermatol 2012;167:1338-44. Doi 10.1111/j.1365-2133.2012.11126.x.
- 31.Zhang X, Gu H, Xie S, Su Y. Periodontitis in patients with psoriasis: A systematic review and meta-analysis. Oral Dis 2022;28(1):33-43. doi: 10.1111/odi.13617.
- 32.Lazaridou E, Tsikrikoni A, Fotiadou C et al. Association of chronic plaque psoriasis and severe periodontitis: a hospital based case-control study. J Eur Acad Dermatol Venereol 2013;27:967-72 doi 10.1111/j.1468-3083.2012.04615.x.
- 33.Ucan Yarkac F, Ogrum A, Gokturk O. Effects of non-surgical periodontal therapy on inflammatory markers of psoriasis: A randomized controlled trial. J Clin Periodontol 2020;47(2):193-201. doi: 10.1111/jcpe.13205.
- 34.González-Álvarez L, García-Martín JM, García-Pola MJ. Association between geographic tongue and psoriasis: A systematic review and meta-analyses. J Oral Pathol Med 2019;48(5):365-72. doi: 10.1111/jop.12840.
- 35.Costa AA, Cota LOM, Mendes VS et al. Impact of oral lesions on the quality of life of psoriatic individuals: A case-control study. Oral Dis 2021;27(7):1813-21. doi: 10.1111/odi.13695.
- 36.Picciani B, Santos T, Domingos C et al. Geographic tongue and fissured tongue in 348 patients with psoriasis: correlation with disease severity. Sci World J 2015;2015:564326.
- 37.Germi L, De Giorgi V, Bergamo F et al. Psoriasis and oral lesions: multicentric study of Oral Mucosa Diseases Italian Group (GIPMO). Dermatol Online J 2012:18(1): 11.
- 38.Talaee R, Hajheydari Z, Moghaddam AY et al. Prevalence of Oral Mucosal Lesions and Their Association with Severity of Psoriasis among Psoriatic Patients Referred To Dermatology Clinic: A Cross-Sectional Study in Kashan/Iran. Open Access Maced J Med Sci 2017;5(7):978-82. doi: 10.3889/oamjms.2017.189.
- 39.Monson CA, Silva V, Porfírio G et al. Oral Health Issues in Psoriasis: An Overview of the Literature. Int J Clin Dermatol & Res 2016;94-103. Doi: 10.19070/2332-2977-1600025.
- 40.Olejnik M, Osmola-Mańkowska A, Ślebioda Z et al. Oral mucosal lesions in psoriatic patients based on disease severity and treatment approach. J Oral Pathol Med 2020;49(8):822-8. doi: 10.1111/jop.13095.
- 41.Zargari O. The prevalence and significance of fissured tongue and geographical tongue in psoriatic patients. Clin and Exper Dermatol 2006;31(2):192-5. doi: 10.1111/j.1365-2230.2005.02028.x.
- 42.Picciani B, Santos VC, Teixeira-Souza T et al. Investigation of the clinical features of geographic tongue: unveiling its relationship with oral psoriasis. Int J Dermatol 2017;56(4):421-7. doi: 10.1111/ijd.13460.
- 43.Picciani BLS, Domingos TA, Teixeira-Souza T et al. Evaluation of the Th17 pathway in psoriasis and geographic tongue. An Bras Dermatol 2019;94(6):677-83. doi: 10.1016/j.abd.2019.01.006.
- 44.National Psoriasis Foundation. Soriatane (Acitretin). https://www.psoriasis.org/soriatane-acitretin/.
- 45.National Psoriasis Foundation. Current Biologics on the Market. https://www.psoriasis.org/current-biologics-on-the-market/.
- 46.Dalmády S, Kemény L, Antal M, Gyulai R. Periodontitis: a newly identified comorbidity in psoriasis and psoriatic arthritis. Expert Rev Clin Immunol 2020;16(1):101-8. doi: 10.1080/1744666X.2019.1700113.