

An Update on Oral Health and Dental Treatment during Pregnancy
Hormonal, vascular and other physiological changes occur during pregnancy that are necessary for fetal development and birth, among them increased production of estrogen and subsequently progesterone, as well as increased production of relaxin.1Lo Giudice R, Martinelli C, Alibrandi A et al. Multicenter Cross-Sectional Study of Oral Health and Hygiene Practices Among Pregnant Women. J Clin Med 2024;13:7315. https://doi.org/10.3390/jcm13237315.,2Napso T, Yong HEJ, Lopez-Tello J, Sferruzzi-Perri AN. The Role of Placental Hormones in Mediating Maternal Adaptations to Support Pregnancy and Lactation. Front Physiol 2018;9:1091. doi:10.3389/fphys.2018.01091. Shifts in the oral environment also occur resulting in potential impacts to oral health and pregnancy outcomes, with a recent study finding that almost 50% of women in their first trimester of pregnancy experience poor oral health.3Robinson JL, Johnson PM, Kister K et al. Estrogen signaling impacts temporomandibular joint and periodontal disease pathology. Odontol 2020;108:153-65. ,4Silva de Araujo Figueiredo C, Gonçalves Carvalho Rosalem C, Costa Cantanhede AL et al. Systemic alterations and their oral manifestations in pregnant women. J Obstet Gynaecol Res 2017;43(1):16-22. doi:10.1111/jog.13150.,5Thomas C, Timofeeva I, Bouchoucha E et al. Oral and periodontal assessment at the first trimester of pregnancy: the PERISCOPE longitudinal study. Acta Obstet Gynecol Scand 2023;102(6):669-80. doi:10.1111/aogs.14529. In this article we will review oral health changes, outcomes, barriers to care and current recommendations.
Salivary changes, dental caries and dental erosion
Hormonal and nutritional changes can result in dry mouth (hyposalivation). This leads to decreased oral clearance, reduced buffering capacity, and reduced supply of minerals, antimicrobial and anti-inflammatory agents from saliva, thereby increasing risk for dental caries and dental erosion, and the lower salivary pH evident during pregnancy favors cariogenic bacteria.4Silva de Araujo Figueiredo C, Gonçalves Carvalho Rosalem C, Costa Cantanhede AL et al. Systemic alterations and their oral manifestations in pregnant women. J Obstet Gynaecol Res 2017;43(1):16-22. doi:10.1111/jog.13150. Furthermore, morning sickness over an extended period lowers the intra-oral pH and can also result in dental erosion.2Napso T, Yong HEJ, Lopez-Tello J, Sferruzzi-Perri AN. The Role of Placental Hormones in Mediating Maternal Adaptations to Support Pregnancy and Lactation. Front Physiol 2018;9:1091. doi:10.3389/fphys.2018.01091. A recent cross-sectional study (n=80) included women experiencing their third trimester of pregnancy, postmenopausal women and younger women who were not pregnant.6Colaco AS, Rai A, Mayya A et al. Impact of hormonal phases on salivary characteristics and oral hygiene in women: a cross-sectional comparative study. BMC Oral Health 2025;26(1):50. doi:10.1186/s12903-025-07284-5. https://doi.org/10.1186/s12903-025-07284-5. After adjusting for age, salivary flow and salivary pH were significantly lower for pregnant and post-menopausal women compared to younger women who were not pregnant. The researchers noted potential confounders including differing oral hygiene levels, socioeconomic status and medication use.
Research results on dental caries during pregnancy have been mixed. In a review of a dataset of pregnant and non-pregnant women 15 to 44 years-of-age from NHANES (2017) data, no differences were found for the overall prevalence of dental caries.7Azofeifa A, Yeung LF, Alverson CJ, Beltrán-Aguilar E. Dental caries and periodontal disease among U.S. pregnant women and nonpregnant women of reproductive age, National Health and Nutrition Examination Survey, 1999–2004. Public Health Dent 2016;76(4):320-9. doi:10.1111/jphd.12159. However, significantly greater levels of dental caries were observed when assessing data restricted to women with lower family income or education levels, with 41% and 23% respectively affected by dental caries.
Periodontal involvement
Pregnancy gingivitis presents as red and swollen gingival tissue that readily bleeds, and affects up to 75% of pregnant women.1Lo Giudice R, Martinelli C, Alibrandi A et al. Multicenter Cross-Sectional Study of Oral Health and Hygiene Practices Among Pregnant Women. J Clin Med 2024;13:7315. https://doi.org/10.3390/jcm13237315.,8Laine MA. Effect of pregnancy on periodontal and dental health. Acta Odontol Scand 2002;60(5):257-64. doi:10.1080/00016350260248210.,9Holmstrup P, Plemons J, Meyle J. Non-plaque-induced gingival diseases. J Clin Periodontol 2018;45 (Suppl. 20):S28-S43. Its development derives from shifts in the oral flora with a greater proportion of periodontopathogens which favors gingivitis, and an elevated immune response while higher levels of estrogen promote gingival enlargement.9Holmstrup P, Plemons J, Meyle J. Non-plaque-induced gingival diseases. J Clin Periodontol 2018;45 (Suppl. 20):S28-S43.,10Lieff S, Boggess KA, Murtha AP et al. The oral conditions and pregnancy study: periodontal status of a cohort of pregnant women. J Periodontol 2004;75:116-26. 10.1902/jop.2004.75.1.116.,11Steinberg B. Women’s oral health issues. J Calif Dent Assoc 2000;28:663-7.,12Raber-Durlacher JE, van Steenbergen TJM, van der Velden U et al. Experimental gingivitis during pregnancy and postpartum: Clinical, endocrinological, and microbiological aspects. J Clin Periodontol 1994;21(8):549-58.,13Gürsoy M, Pajukanta R, Sorsa T, Könönen E: Clinical changes in periodontium during pregnancy and post-partum. J Clin Periodontol 2008;35:576-83. 10.1111/j.1600-051X.2008.01236.x. The onset of pregnancy gingivitis can occur in the first three months and, in the absence of intervention, can increase in severity throughout pregnancy. While not common, periodontitis may develop,14Moss KL, Beck JD, Offenbacher S. Clinical risk factors associated with incidence and progression of periodontal conditions in pregnant women. J Clin Periodontol 2005;32:492-8. and results from a recent systematic review and meta-analysis suggest that periodontitis doubles the risk for gestational diabetes mellitus.15Abariga SA, Whitcomb BW. Periodontitis and gestational diabetes mellitus: a systematic review and meta-analysis of observational studies. BMC Pregnancy Childbirth 2016;16(1):344. doi:10.1186/s12884-016-1145-z. Pregnancy epulis (pregnancy-associated pyogenic granulomas) may develop during pregnancy, with a reported prevalence of up to 10%, and are most common during the third trimester.9Holmstrup P, Plemons J, Meyle J. Non-plaque-induced gingival diseases. J Clin Periodontol 2018;45 (Suppl. 20):S28-S43.,14Moss KL, Beck JD, Offenbacher S. Clinical risk factors associated with incidence and progression of periodontal conditions in pregnant women. J Clin Periodontol 2005;32:492-8. (Figure 1) Gingival changes normally resolve post-partum provided that local irritants are removed.8Laine MA. Effect of pregnancy on periodontal and dental health. Acta Odontol Scand 2002;60(5):257-64. doi:10.1080/00016350260248210. Lastly, temporary tooth mobility accompanied by clinical attachment loss can occur as a direct result of increased levels of relaxin produced during pregnancy to loosen the mother's pelvic ligaments prior to childbirth.16Scheutz F, Baelum V, Matee MI, Mwangosi I. Motherhood and dental disease. Comm Dent Health 2002;19(2):67-72.
Figure 1. Clinical presentation of a pyogenic granuloma

Source: Zahid E, Bhatti O, Zahid MA, Stubbs M. Overview of common oral lesions. doi: 10.51866/rv.37. (CC BY 4.0)
Findings on maternal periodontitis and adverse pregnancy outcomes
Results of umbrella reviews, systematic reviews and meta-analyses have demonstrated associations/relationships between periodontitis during pregnancy and adverse pregnancy outcomes (APO), including low-birth-weight babies, premature birth and pre-eclampsia.17Arabzadeh H, Doosti-Irani A, Kamkari S et al. The maternal factors associated with infant low birth weight: an umbrella review. BMC Pregnancy Childbirth 2024;24(1):316. doi:10.1186/s12884-024-06487-y.,18Daalderop LA, Wieland BV, Tomsin K et al. Periodontal Disease and Pregnancy Outcomes: Overview of Systematic Reviews. JDR Clin Trans Res 2018;3(1):10-27.,19Manrique-Corredor EJ, Orozco-Beltran D, Lopez-Pineda A et al. Maternal periodontitis and preterm birth: Systematic review and meta-analysis. Community Dent Oral Epidemiol 2019;47(3):243-51. doi: 10.1111/cdoe.12450.,20Alnasser BH, Alkhaldi NK, Alghamdi WK, Alghamdi FT. The Potential Association Between Periodontal Diseases and Adverse Pregnancy Outcomes in Pregnant Women: A Systematic Review of Randomized Clinical Trials. Cureus 2023;15(1):e33216. doi: 10.7759/cureus.33216.,21Le QA, Akhter R, Coulton KM et al. Periodontitis and Preeclampsia in Pregnancy: A Systematic Review and Meta-Analysis. Matern Child Health J 2022;26(12):2419-43. doi: 10.1007/s10995-022-03556-6. In an umbrella review conducted in 2024 that included 13 systematic reviews and 15 meta-analyses, it was found that maternal periodontitis resulted in a more than two-fold risk for low birth weight babies.15Abariga SA, Whitcomb BW. Periodontitis and gestational diabetes mellitus: a systematic review and meta-analysis of observational studies. BMC Pregnancy Childbirth 2016;16(1):344. doi:10.1186/s12884-016-1145-z. This exceeded the increases in risk levels found for hypertension or use of cocaine/crack cocaine. Other risk factors identified included anemia, hypothyroidism, alcohol use, smoking, depression, being underweight and work with heavy physical loads. In a second umbrella review (2023) with a meta-analysis of 7 systematic reviews, the researchers reported an association between maternal periodontitis and elevated risk for low birth weight and premature babies.22Padilla-Cáceres T, Arbildo-Vega HI, Caballero-Apaza L et al. Association between the Risk of Preterm Birth and Low Birth Weight with Periodontal Disease in Pregnant Women: An Umbrella Review. Dent J (Basel) 2023;11(3):74. doi:10.3390/dj11030074. In an earlier umbrella review (2018) with 23 systematic reviews, maternal periodontitis was again found to be associated with APO, including pre-eclampsia. However, for some studies no associations between maternal periodontitis and APO have been found.23Choi SE, Choudhary A, Ahern JM et al. Association between maternal periodontal disease and adverse pregnancy outcomes: an analysis of claims data. Fam Pract 2021;38:718-23. doi:10.1093/fampra/cmab037.,24Teshome A, Yitayeh A. Relationship between periodontal disease and preterm low birth weight: systematic review. Pan Afr Med J 2016;24:215. doi:10.11604/pamj.2016.24.215.8727. Conflicting results have been attributed to factors related to study design, such as small sample sizes and individual factors in the studied population group.
Results from insurance claims data
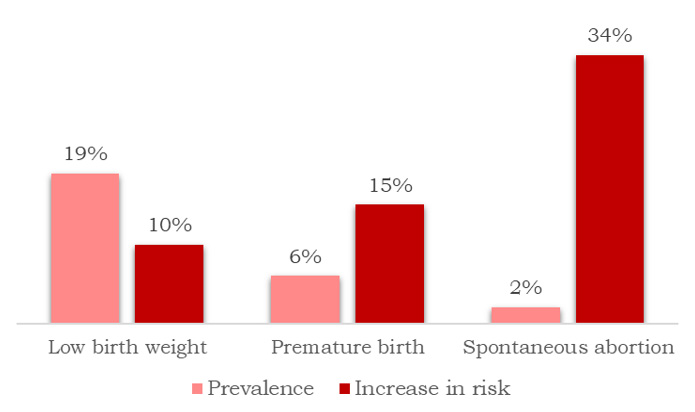
Based on a large dataset of de-identified claims dataset from a national insurance company, for pregnancies occurring between 2015 through 2019 approximately 18.7%, 5.9% and 2.2%, respectively, resulted in low birth weight, premature birth, and spontaneous abortion.23Choi SE, Choudhary A, Ahern JM et al. Association between maternal periodontal disease and adverse pregnancy outcomes: an analysis of claims data. Fam Pract 2021;38:718-23. doi:10.1093/fampra/cmab037. After adjusting for other individual risk factors, maternal periodontitis was determined to increase risk for these conditions by 10%, 15% and 34%, respectively. (Figure 2)
Figure 2. Prevalence of APO and increased risk associated with maternal periodontitis
Proposed mechanisms for the association between periodontitis and APO
The proposed mechanisms for the relationship between periodontitis and APO include a dental bacteremia that occurs when oral microorganisms enter the circulation which is enabled by the increased vascularity and permeability of the gingival tissue during pregnancy, and after which the microorganisms reach the placenta and trigger an inflammatory response.25Butera A, Maiorani C, Morandini A et al. Periodontitis in Pregnant Women: A Possible Link to Adverse Pregnancy Outcomes. Healthcare (Basel) 2023;11(10):1372. doi:10.3390/healthcare11101372. It is also hypothesized that the oral bacteria may promote systemic inflammation that increases risk for APO, and that inflammatory responses may induce oxidative stress and endothelial dysfunction systemically.26Parry S, Jeffcoat M, Reddy MS et al. Evaluation of an advanced oral hygiene regimen on maternity outcomes in a randomized multicenter clinical trial (Oral Hygiene and Maternity Outcomes Multicenter Study). Am J Obstet Gynecol MFM 2023;5:100995.,27Patel N. The Impact of Periodontal Disease on Adverse Pregnancy Outcomes: A Comprehensive Review 21st World Congress in Fetal Medicine (Lisbon, Portugal; June, 2024).
Current Recommendations for Dental Care during Pregnancy
Current recommendations in the United States are based on a consensus statement that was jointly developed in 2011 by representatives from the American Dental Association (ADA), American College of Obstetricians and Gynecologists (ACOG) and the Health Resources and Services Administration's Maternal and Child Health Bureau at a meeting convened by the National Maternal and Child Oral Health Resource Center.28American College of Obstetricians and Gynecologists. Oral Health Care During Pregnancy and Through the Lifespan. Committee Opinion, Number 569, August 2013. Reaffirmed 2025. https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2013/08/oral-health-care-during-pregnancy-and-through-the-lifespan. ,29Oral Health Care During Pregnancy Expert Workgroup. 2026. Oral Health Care During Pregnancy: A National Consensus Statement (rev. ed.). Washington, DC: National Maternal and Child Oral Health Resource Center. https://www.mchoralhealth.org/PDFs/OralHealthPregnancyConsensus.pdf#. This consensus statement has continued to be reviewed, and was reaffirmed in 2025.28American College of Obstetricians and Gynecologists. Oral Health Care During Pregnancy and Through the Lifespan. Committee Opinion, Number 569, August 2013. Reaffirmed 2025. https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2013/08/oral-health-care-during-pregnancy-and-through-the-lifespan. ,30Bao J, Huang X, Wang L et al. Clinical practice guidelines for oral health care during pregnancy: a systematic evaluation and summary recommendations for general dental practitioners. Quintessence Int 2022;53(4):362-373. doi:10.3290/j.qi.b2644863. In addition, in 2024 the ADA adopted a statement titled 'Comprehensive Statement on Oral Health Services During Pregnancy'.31American Dental Association. Pregnancy. https://www.ada.org/resources/ada-library/oral-health-topics/pregnancy. The reader should consult these documents for full information on current recommendations, including on procedures, medication use and instructions during pregnancy.
Key elements of the recommendations
Based on current recommendations, all women should receive a full oral evaluation (including dental and medical history) and risk assessment, oral hygiene instructions and dietary advice, and preventive care and diagnostic procedures are considered safe throughout pregnancy, including dental radiographs.28American College of Obstetricians and Gynecologists. Oral Health Care During Pregnancy and Through the Lifespan. Committee Opinion, Number 569, August 2013. Reaffirmed 2025. https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2013/08/oral-health-care-during-pregnancy-and-through-the-lifespan. ,29Oral Health Care During Pregnancy Expert Workgroup. 2026. Oral Health Care During Pregnancy: A National Consensus Statement (rev. ed.). Washington, DC: National Maternal and Child Oral Health Resource Center. https://www.mchoralhealth.org/PDFs/OralHealthPregnancyConsensus.pdf#. ,30Bao J, Huang X, Wang L et al. Clinical practice guidelines for oral health care during pregnancy: a systematic evaluation and summary recommendations for general dental practitioners. Quintessence Int 2022;53(4):362-373. doi:10.3290/j.qi.b2644863.,31American Dental Association. Pregnancy. https://www.ada.org/resources/ada-library/oral-health-topics/pregnancy. As with all patients, indicated dental radiographs should always be taken with the patient wearing a thyroid collar and protective apron and in accordance with the ALARA principle (i.e., radiation exposure As Low As Reasonably Achievable).31American Dental Association. Pregnancy. https://www.ada.org/resources/ada-library/oral-health-topics/pregnancy. ,32American Dental Association. Radiographic Imaging, 2026. https://www.ada.org/resources/practice/practice-management/radiographic-imaging. In addition, as indicated, other routine treatments are recommended throughout pregnancy, including restorative, endodontic and periodontal procedures.31American Dental Association. Pregnancy. https://www.ada.org/resources/ada-library/oral-health-topics/pregnancy. Of note, while risk of bias has been noted in systematic reviews on periodontal therapy and APO, periodontal therapy does not adversely affect pregnancy outcomes and it does improve maternal oral health.28American College of Obstetricians and Gynecologists. Oral Health Care During Pregnancy and Through the Lifespan. Committee Opinion, Number 569, August 2013. Reaffirmed 2025. https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2013/08/oral-health-care-during-pregnancy-and-through-the-lifespan. Emergency dental procedures (e.g., extractions or endodontic treatment) during pregnancy are also considered safe.28American College of Obstetricians and Gynecologists. Oral Health Care During Pregnancy and Through the Lifespan. Committee Opinion, Number 569, August 2013. Reaffirmed 2025. https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2013/08/oral-health-care-during-pregnancy-and-through-the-lifespan. ,31American Dental Association. Pregnancy. https://www.ada.org/resources/ada-library/oral-health-topics/pregnancy. (Table 1)
| Table 1. Current recommendations on dental treatment |
|---|
| Full oral evaluation, including dental and medical history and risk assessment |
| Advice on oral hygiene and diet during pregnancy |
| Preventive care |
| Diagnostic procedures, including indicated dental radiographs (and ALARA) |
| Routine treatment, incl. restorative, endodontic and periodontal procedures |
| Emergency treatment - endodontic therapy and extractions |
Medications include but are not limited to local anesthetics, analgesics and sedation agents. A local anesthetic containing epinephrine is considered safe when indicated, and suggested antibiotics include penicillin, amoxicillin, cephalosporins, clindamycin and metronidazole (provided not contraindicated for an individual patient, e.g., due to allergies).31American Dental Association. Pregnancy. https://www.ada.org/resources/ada-library/oral-health-topics/pregnancy. All other classes of antibiotics should be avoided during pregnancy.29Oral Health Care During Pregnancy Expert Workgroup. 2026. Oral Health Care During Pregnancy: A National Consensus Statement (rev. ed.). Washington, DC: National Maternal and Child Oral Health Resource Center. https://www.mchoralhealth.org/PDFs/OralHealthPregnancyConsensus.pdf#. Additionally, the consensus from the Oral Health Care During Pregnancy Expert Workgroup (2026) states that acetaminophen may be used throughout pregnancy, while aspirin, ibuprofen and naproxen should be avoided during the first and third trimesters.29Oral Health Care During Pregnancy Expert Workgroup. 2026. Oral Health Care During Pregnancy: A National Consensus Statement (rev. ed.). Washington, DC: National Maternal and Child Oral Health Resource Center. https://www.mchoralhealth.org/PDFs/OralHealthPregnancyConsensus.pdf#. During the second trimester, specific and limited use of analgesics is recommended. Analgesic use should be determined in collaboration with the patient's obstetrician, and the patients obstetrician needs to be consulted prior to any proposed use of nitrous oxide (i.e., oral sedation or as an adjunctive analgesic), or intravenous sedation or general anesthetics, to determine whether this is appropriate and safe.29Oral Health Care During Pregnancy Expert Workgroup. 2026. Oral Health Care During Pregnancy: A National Consensus Statement (rev. ed.). Washington, DC: National Maternal and Child Oral Health Resource Center. https://www.mchoralhealth.org/PDFs/OralHealthPregnancyConsensus.pdf#. ,30Bao J, Huang X, Wang L et al. Clinical practice guidelines for oral health care during pregnancy: a systematic evaluation and summary recommendations for general dental practitioners. Quintessence Int 2022;53(4):362-373. doi:10.3290/j.qi.b2644863.,31American Dental Association. Pregnancy. https://www.ada.org/resources/ada-library/oral-health-topics/pregnancy.
Outcomes from studies on periodontal treatment and APO
A recent systematic review ( 2025) included 24 randomized controlled trials (RCT), with studies investigating the effects of scaling and root planing, oral hygiene instruction and adjunctive use of antimicrobial rinses on APO.33Anas M, Sultan MU, Fazal A. et al. Impact of periodontal therapy on adverse pregnancy outcomes: a systematic review of randomized controlled trials. Perio Implant Res 2025; 9:17. https://doi.org/10.1007/s41894-025-00161-y. Study results were conflicting, while no reduction in APO was observed in the large multi-center trials. A Cochrane review ( 2017) included 15 RCT with more than 7,000 pregnant women, with 14 RCT focused on periodontitis and one on gingivitis.34Iheozor-Ejiofor Z, Middleton P, Esposito M, Glenny AM. Treating periodontal disease for preventing adverse birth outcomes in pregnant women. Cochrane Database Syst Rev 2017;6:CD005297. doi:10.1002/14651858.CD005297.pub3. The researchers concluded that a low level of evidence existed that periodontal treatment during pregnancy may reduce low birth weight babies. However, it was unclear whether treatment had any effect on premature birth and insufficient evidence on the most favorable treatment method to prevent APO. Earlier meta-analysis had led to similar conclusions, with a lack of clarity on whether periodontal treatment had any impact on risk for preeclampsia.28American College of Obstetricians and Gynecologists. Oral Health Care During Pregnancy and Through the Lifespan. Committee Opinion, Number 569, August 2013. Reaffirmed 2025. https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2013/08/oral-health-care-during-pregnancy-and-through-the-lifespan.
In a recent RCT with more than 600 participants with moderate to severe gingivitis, one group received only mechanical debridement while the other group also received robust oral hygiene instructions and used a power brush with an antibacterial toothpaste, flossed and rinsed with an antibacterial mouthwash.26Parry S, Jeffcoat M, Reddy MS et al. Evaluation of an advanced oral hygiene regimen on maternity outcomes in a randomized multicenter clinical trial (Oral Hygiene and Maternity Outcomes Multicenter Study). Am J Obstet Gynecol MFM 2023;5:100995. While no statistically significant differences in the rates of premature birth were found overall, the rate was statistically significantly lower for pregnant women who were socioeconomically disadvantaged.
Dental Visit Utilization
Current guidelines are clear on the need for dental care and its safety during pregnancy, however up to at least 50% of pregnant women do not visit a dental professional and in one report the researchers found that less than a fifth had visited a dentist in the prior six months.1Lo Giudice R, Martinelli C, Alibrandi A et al. Multicenter Cross-Sectional Study of Oral Health and Hygiene Practices Among Pregnant Women. J Clin Med 2024;13:7315. https://doi.org/10.3390/jcm13237315.,35Ramanauskaite E, Maciulskiene V, Baseviciene N, Anuzyte R. A Survey of Lithuanian Pregnant Women’s Knowledge about Periodontal Disease, Its Prevalence and Possible Influence on Pregnancy Outcomes. Medicina 2024;60:1431. https://doi.org/10.3390/medicina60091431.,36Naavaal S, Brickhouse TH, Hafidh S, Smith K. Factors Associated with Preventive Dental Visits Before and During Pregnancy. J Womens Health (Larchmt) 2019;28(12):1670-8. doi:10.1089/jwh.2018.7509. The Pregnancy Risk Assessment Monitoring System (PRAMS) surveys, conducted periodically in US states, provide insights on oral care advice and dental visits during pregnancy. In the Texas PRAMS survey published in 2018 (data from 2012-2015), approximately 36% of pregnant women received a prophylaxis.37Texas Health and Human Services. Pregnancy Risk Assessment Monitoring System (PRAMS) Survey 2018 Data Book: Summary Tables. https://www.dshs.texas.gov/sites/default/files/mch/pdf/2018-PRAMS-Databook.pdf. Based on results from the Rhode Island PRAMS survey for the same time period, approximately 57% and 62% of individuals received a prophylaxis during their latest pregnancy, with differences in the percentage of pregnant women receiving/not receiving a prophylaxis found to be related to specific attributes.38Chenwi H, Savitz D. Distribution of Preventive Dental Care during pregnancy in Rhode Island, 2012 to 2015. Rhode Island Medical Journal 2018:19-22. http://rimed.org/rimedicaljournal/2018/11/2018-11-19-cont-chenwi.pdf. Risk factors included whether the pregnancy was unintended, and whether the individual had received prenatal care or had relocated more than once in the prior three years. Furthermore, approximately 23% received prophylaxis if their dentist or other healthcare professional had not discussed oral care, compared to 77% when this had been discussed.
In one study on women who had given birth in the prior 2 years, just 56% were aware of the correlation between poor oral health and APO, and only 10% and 11% of these women, respectively, were educated on this by their dental office or obstetrician.39Azarshahri A, Rainchuso L, Vineyard J, Giblin-Scanlon L. Postpartum U.S. Women's Oral Health Knowledge, Attitudes, and Practices During Pregnancy. Matern Child Health J 2022;26(6):1339-49. doi:10.1007/s10995-021-03326-w. Additionally, in a recent survey among medical professionals, only 6% always obtained an oral health history and 7% included a dental screening during patients' pre-natal care.40Hoerler SB, Jenkins S, Assad D. Evaluating Oral Health in Pregnant Women: Knowledge, attitudes and practices of health professionals . J Dent Hyg 2019;93(1):16-22.
Barriers to Dental Treatment during Pregnancy
Barriers to dental visits and treatment include misperceptions/myths among pregnant women, acceptance that oral health problems are 'normal' during pregnancy, negative perceptions of dental care, fear of treatment, potential discomfort when seated in the dental chair, fear of vomiting during a dental visit, treatment costs, lack of information, poor advice, lack of support, transportation difficulties and other constraints.41Rocha JS, Arima L, Chibinski AC et al. Barriers and facilitators to dental care during pregnancy: a systematic review and meta-synthesis of qualitative studies. Cad Saúde Pública 2018;34:e00130817. doi:10.1590/0102-311X00130817.,42Kamalabadi YM, Campbell MK, Zitoun NM et al. Unfavourable beliefs about oral health and safety of dental care during pregnancy: a systematic review. BMC Oral Health 2023;23:762. https://doi.org/10.1186/s12903-023-03439-4.,43George A, Johnson M, Duff M et al. Midwives and oral health care during pregnancy: perceptions of pregnant women in south-western Sydney, Australia. J Clin Nurs 2012;21(7-8):1087-96. doi:10.1111/j.1365-2702.2011.03870.x. ,44Ebinghaus M, Agricola CJ, Schmittinger J et al. Assessment of women's needs and wishes regarding interprofessional guidance on oral health in pregnancy - a qualitative study. BMC Pregnancy Childbirth 2024;24(1):471. doi:10.1186/s12884-024-06675-w. (Table 2)
| Table 2. Patient barriers to dental treatment during pregnancy |
|---|
| Misperceptions/myths |
| Acceptance that oral health problems are 'normal' |
| Negative perceptions of dental care |
| Fear of treatment |
| Fear of vomiting during a dental visit |
| Treatment costs |
| Lack of information |
| Poor advice |
| Support/lack of support |
| Transport difficulties |
| Other constraints |
Misperceptions/myths
Misperceptions regarding dental treatment during pregnancy are common, and in a systematic review with 45 studies four areas were explored.42Kamalabadi YM, Campbell MK, Zitoun NM et al. Unfavourable beliefs about oral health and safety of dental care during pregnancy: a systematic review. BMC Oral Health 2023;23:762. https://doi.org/10.1186/s12903-023-03439-4. In approximately 12 of 35 studies, pregnant women perceived that dental treatment was unsafe during pregnancy. Specific types of treatment were perceived as unsafe among subjects in 12 studies, and noted perceptions included that dental radiographs and radiation exposure were harmful to the fetus. In eight studies, dental (local) anesthesia was considered hazardous, with 25% to 95% of participants believing this depending on the study, while in a further four studies pregnant women believed that pain medications were hazardous to the fetus and in other studies that dental extraction was harmful. Similar findings and misperceptions were found in an earlier systematic review.41Rocha JS, Arima L, Chibinski AC et al. Barriers and facilitators to dental care during pregnancy: a systematic review and meta-synthesis of qualitative studies. Cad Saúde Pública 2018;34:e00130817. doi:10.1590/0102-311X00130817.
Additional misperceptions that have been reported include that restorative care, scaling and prophylaxis and periodontal therapy are unsafe. In a more recent survey conducted in Ontario, Canada with 130 subjects 18 years-of-age and older, approximately half of the participants believed that dental treatment impacts the health of the fetus, with similar beliefs reported about potential harms from radiographs, analgesics and antibiotics.45Kamalabadi YM, Campbell MK, Gratton R et al. Oral health-related beliefs among a sample of pregnant women in Southwestern Ontario: a descriptive study. Front Oral Health 2024;5:1485815. doi:10.3389/froh.2024.1485815. In addition, almost two-thirds believed that pregnancy affected their oral health (loss of calcium and other negative impacts). Loss of calcium from maternal teeth to provide calcium for fetal development, and loss of teeth, are noted in numerous studies as misperceptions among pregnant women.41Rocha JS, Arima L, Chibinski AC et al. Barriers and facilitators to dental care during pregnancy: a systematic review and meta-synthesis of qualitative studies. Cad Saúde Pública 2018;34:e00130817. doi:10.1590/0102-311X00130817.,42Kamalabadi YM, Campbell MK, Zitoun NM et al. Unfavourable beliefs about oral health and safety of dental care during pregnancy: a systematic review. BMC Oral Health 2023;23:762. https://doi.org/10.1186/s12903-023-03439-4.,46Al‐Swuailem AS. Knowledge of periodontal disease in expecting mothers and its association with utilization of dental services in Riyadh, Saudi Arabia. Pak Oral Dent J 2015;35(2):238-43.,47Velosa‐Porras J, Rodríguez Malagón, N. Perceptions, knowledge, and practices related to oral health in a group of pregnant women: A qualitative study. Clin Exp Dent Res 2024;10:e823. https://doi.org/10.1002/cre2.823.
Barriers to the provision of oral care among healthcare professionals
Barriers to the provision of oral care by healthcare professionals in clinical practice and teaching institutions include lack of knowledge, limited clinical experience, fear of liability, and lack of faculty experience in dental schools due to the limited number of pregnant patients which also results in less education and experience for students.44Ebinghaus M, Agricola CJ, Schmittinger J et al. Assessment of women's needs and wishes regarding interprofessional guidance on oral health in pregnancy - a qualitative study. BMC Pregnancy Childbirth 2024;24(1):471. doi:10.1186/s12884-024-06675-w.,48Rasubala L, Russell SL, Ren Y et al. Dental Faculty Knowledge, Attitudes, and Willingness to Treat Pregnant Persons at 2 Institutions. JDR Clin Trans Res 2025;10(Suppl 1):58S-66S. doi:10.1177/23800844251328637.,49Huang SS, Yang C, Cohen V, Russell SL. What Factors Influence Dental Faculty's Willingness to Treat Pregnant Women? JDR Clin Trans Res 2022;7(4):407-14. doi: 10.1177/23800844211028132.
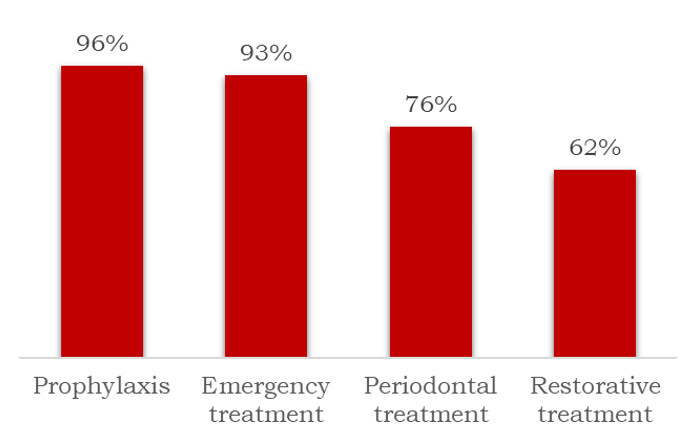
In a survey of members of the Michigan Dental Hygiene Association (2016), 90% of responding dental hygienists reported willingness to treat pregnant women and 85% knew that dental hygiene care can be provided throughout pregnancy.50Schramm SA, Jacks ME, Prihoda TJ et al. Oral Care for Pregnant Patients: A Survey of Dental Hygienists' Knowledge, Attitudes and Practice. J Dent Hyg 2016;90(2):121-7. However, awareness of current recommendations for specific procedures varied, with approximately 96%, 93%, 76% and 62%, respectively believing that prophylaxis, emergency treatment, periodontal treatment and restorative care could be provided throughout pregnancy.50Schramm SA, Jacks ME, Prihoda TJ et al. Oral Care for Pregnant Patients: A Survey of Dental Hygienists' Knowledge, Attitudes and Practice. J Dent Hyg 2016;90(2):121-7. (Figure 3) In a survey conducted the same year in France among dentists, obstetricians and midwives, a high level of knowledge was found for pregnancy gingivitis and relationship between periodontitis and low birth weight or premature birth, while midwives and obstetricians lacked knowledge of pregnancy epulis.51Boutigny H, de Moegen M-L, Egea L et al. Oral Infections and Pregnancy: Knowledge of Gynecologists/Obstetricians, Midwives and Dentists. Oral Health Prev Dent 2016;14(1):41-7. doi:10.3290/j.ohpd.a34376.
Figure 3. Percentage of dental hygienists regarding specific procedures as safe during pregnancy50Schramm SA, Jacks ME, Prihoda TJ et al. Oral Care for Pregnant Patients: A Survey of Dental Hygienists' Knowledge, Attitudes and Practice. J Dent Hyg 2016;90(2):121-7.
Among dental faculty in one dental school, results of a cross-sectional survey conducted in 2025 showed that 90% of respondents (n=65) agreed that pregnant women should visit the dentist, while fewer than half knew of the guidelines on dental treatment and oral care during pregnancy.48Rasubala L, Russell SL, Ren Y et al. Dental Faculty Knowledge, Attitudes, and Willingness to Treat Pregnant Persons at 2 Institutions. JDR Clin Trans Res 2025;10(Suppl 1):58S-66S. doi:10.1177/23800844251328637. Approximately a fifth of respondents were also concerned about potential liability which translated to a five-fold likelihood of unwillingness to treat pregnant patients. In an earlier survey conducted four years earlier in the largest US dental school, 80% of the clinical faculty believed pregnant women should see a dentist while only 40% were aware of the same guidelines, and 30% were concerned about potential liability.49Huang SS, Yang C, Cohen V, Russell SL. What Factors Influence Dental Faculty's Willingness to Treat Pregnant Women? JDR Clin Trans Res 2022;7(4):407-14. doi: 10.1177/23800844211028132. Dental and other healthcare professionals responding to surveys consistently report a desire for more knowledge and continuing education on oral care and dental considerations during pregnancy.48Rasubala L, Russell SL, Ren Y et al. Dental Faculty Knowledge, Attitudes, and Willingness to Treat Pregnant Persons at 2 Institutions. JDR Clin Trans Res 2025;10(Suppl 1):58S-66S. doi:10.1177/23800844251328637.,50Schramm SA, Jacks ME, Prihoda TJ et al. Oral Care for Pregnant Patients: A Survey of Dental Hygienists' Knowledge, Attitudes and Practice. J Dent Hyg 2016;90(2):121-7.,52AlHalal H, Albayyat R M, Alfhaed N K et al. Knowledge, Attitude, and Practice Regarding Periodontal and Dental Diseases During Pregnancy Among Obstetricians and Dentists in King Saud University Medical City. Cureus 2023;15(10): e47098. doi:10.7759/cureus.47098.,53Naavaal S, Claiborne DM. Oral Health Knowledge, Practices, and Awareness of Oral Health Guidelines and Dental Coverage Policies among Midwives. J Midwifery Womens Health 2021;66(1):88-95. doi:10.1111/jmwh.13191.,54George A, Ajwani S, Bhole S et al. Knowledge, attitude and practises of dentists towards oral health care during pregnancy: A cross sectional survey in New South Wales, Australia. Aust Dent J 2017;62(3):301-10. doi: 10.1111/adj.12505.
Implications for Dental Professionals
Dental professionals should always advise patients to perform thorough oral hygiene twice-daily using a soft toothbrush and fluoridated toothpaste, and to perform interdental cleaning once daily.31American Dental Association. Pregnancy. https://www.ada.org/resources/ada-library/oral-health-topics/pregnancy. In-office preventives may also be indicated. In addition, use of alcohol-free chlorhexidine gluconate or cetylpyridinum chloride rinses is also recommended.28American College of Obstetricians and Gynecologists. Oral Health Care During Pregnancy and Through the Lifespan. Committee Opinion, Number 569, August 2013. Reaffirmed 2025. https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2013/08/oral-health-care-during-pregnancy-and-through-the-lifespan. Patients experiencing morning sickness or more serious vomiting during pregnancy can be advised to rinse with a cup of water containing 1 teaspoon of dissolved baking dose after vomiting to help combat and remove gastric acid. In addition, it is important to educate women on oral health challenges and the association between maternal periodontitis and APO to improve knowledge and understanding (and may also encourage appropriate oral hygiene). Patients should be advised that dental visits and treatment are safe and important during pregnancy and educated on the need for thorough oral hygiene during pregnancy to reduce the transfer of Streptococcus mutans to their offspring after their birth and advised before delivery on caring for their infants oral health.
Additionally, given that some pregnant women may be uncomfortable when seated in the dental chair, particularly during the third trimester, reassurance that the most comfortable position possible will be selected with their input can help to encourage dental visits. Recommendations in this regard include using a semi-reclined position, placing a small pillow under the right hip as indicated for comfort, and allowing for position changes during treatment.29Oral Health Care During Pregnancy Expert Workgroup. 2026. Oral Health Care During Pregnancy: A National Consensus Statement (rev. ed.). Washington, DC: National Maternal and Child Oral Health Resource Center. https://www.mchoralhealth.org/PDFs/OralHealthPregnancyConsensus.pdf#.
Conclusions
During pregnancy, systemic changes impact the oral environment, which can result in harm to oral health and for maternal periodontitis has the potential to increase risk for APO. While current guidelines provide information for dental and healthcare professionals, and information is available for women, there are significant gaps in knowledge among pregnant patients with many misperceptions on dental treatment and its safety during pregnancy. In addition, knowledge, and training on dental treatment during pregnancy is suboptimal among dental professionals, obstetricians, and midwives. Dental visit utilization may be increased by educating women on the safety and need for dental treatment and dispelling misperceptions. However, more continuing education on treating pregnant patients is consistently requested in studies with healthcare personnel, including dental professionals in practice and dental faculty in schools. In addition, interprofessional collaboration is limited and should be increased, as it is necessary for optimal safe treatment and would be helpful in educating across disciplines for the promotion of oral health to ultimately benefit patients.33Anas M, Sultan MU, Fazal A. et al. Impact of periodontal therapy on adverse pregnancy outcomes: a systematic review of randomized controlled trials. Perio Implant Res 2025; 9:17. https://doi.org/10.1007/s41894-025-00161-y.,55Skvoretz J, Dyer K, Daley E et al. Research and Practice Communications Between Oral Health Providers and Prenatal Health Providers: A Bibliometric Analysis. Matern Child Health J 2016 Aug;20(8):1607-19. doi: 10.1007/s10995-016-1960-x. It has also been noted by researchers that more studies designed as robust RCT are required to determine an association between maternal periodontitis and APO, and to investigate the potential effect of pre-natal periodontal therapy on APO.23Choi SE, Choudhary A, Ahern JM et al. Association between maternal periodontal disease and adverse pregnancy outcomes: an analysis of claims data. Fam Pract 2021;38:718-23. doi:10.1093/fampra/cmab037.,24Teshome A, Yitayeh A. Relationship between periodontal disease and preterm low birth weight: systematic review. Pan Afr Med J 2016;24:215. doi:10.11604/pamj.2016.24.215.8727.,56Bostanci N. Periodontal health and pregnancy outcomes: time to deliver. Acta Obstet Gynecol Scand 2023;102:648-51. 10.1111/aogs.14548.
References
- 1.Lo Giudice R, Martinelli C, Alibrandi A et al. Multicenter Cross-Sectional Study of Oral Health and Hygiene Practices Among Pregnant Women. J Clin Med 2024;13:7315. https://doi.org/10.3390/jcm13237315.
- 2.Napso T, Yong HEJ, Lopez-Tello J, Sferruzzi-Perri AN. The Role of Placental Hormones in Mediating Maternal Adaptations to Support Pregnancy and Lactation. Front Physiol 2018;9:1091. doi:10.3389/fphys.2018.01091.
- 3.Robinson JL, Johnson PM, Kister K et al. Estrogen signaling impacts temporomandibular joint and periodontal disease pathology. Odontol 2020;108:153-65.
- 4.Silva de Araujo Figueiredo C, Gonçalves Carvalho Rosalem C, Costa Cantanhede AL et al. Systemic alterations and their oral manifestations in pregnant women. J Obstet Gynaecol Res 2017;43(1):16-22. doi:10.1111/jog.13150.
- 5.Thomas C, Timofeeva I, Bouchoucha E et al. Oral and periodontal assessment at the first trimester of pregnancy: the PERISCOPE longitudinal study. Acta Obstet Gynecol Scand 2023;102(6):669-80. doi:10.1111/aogs.14529.
- 6.Colaco AS, Rai A, Mayya A et al. Impact of hormonal phases on salivary characteristics and oral hygiene in women: a cross-sectional comparative study. BMC Oral Health 2025;26(1):50. doi:10.1186/s12903-025-07284-5. https://doi.org/10.1186/s12903-025-07284-5.
- 7.Azofeifa A, Yeung LF, Alverson CJ, Beltrán-Aguilar E. Dental caries and periodontal disease among U.S. pregnant women and nonpregnant women of reproductive age, National Health and Nutrition Examination Survey, 1999–2004. Public Health Dent 2016;76(4):320-9. doi:10.1111/jphd.12159.
- 8.Laine MA. Effect of pregnancy on periodontal and dental health. Acta Odontol Scand 2002;60(5):257-64. doi:10.1080/00016350260248210.
- 9.Holmstrup P, Plemons J, Meyle J. Non-plaque-induced gingival diseases. J Clin Periodontol 2018;45 (Suppl. 20):S28-S43.
- 10.Lieff S, Boggess KA, Murtha AP et al. The oral conditions and pregnancy study: periodontal status of a cohort of pregnant women. J Periodontol 2004;75:116-26. 10.1902/jop.2004.75.1.116.
- 11.Steinberg B. Women’s oral health issues. J Calif Dent Assoc 2000;28:663-7.
- 12.Raber-Durlacher JE, van Steenbergen TJM, van der Velden U et al. Experimental gingivitis during pregnancy and postpartum: Clinical, endocrinological, and microbiological aspects. J Clin Periodontol 1994;21(8):549-58.
- 13.Gürsoy M, Pajukanta R, Sorsa T, Könönen E: Clinical changes in periodontium during pregnancy and post-partum. J Clin Periodontol 2008;35:576-83. 10.1111/j.1600-051X.2008.01236.x.
- 14.Moss KL, Beck JD, Offenbacher S. Clinical risk factors associated with incidence and progression of periodontal conditions in pregnant women. J Clin Periodontol 2005;32:492-8.
- 15.Abariga SA, Whitcomb BW. Periodontitis and gestational diabetes mellitus: a systematic review and meta-analysis of observational studies. BMC Pregnancy Childbirth 2016;16(1):344. doi:10.1186/s12884-016-1145-z.
- 16.Scheutz F, Baelum V, Matee MI, Mwangosi I. Motherhood and dental disease. Comm Dent Health 2002;19(2):67-72.
- 17.Arabzadeh H, Doosti-Irani A, Kamkari S et al. The maternal factors associated with infant low birth weight: an umbrella review. BMC Pregnancy Childbirth 2024;24(1):316. doi:10.1186/s12884-024-06487-y.
- 18.Daalderop LA, Wieland BV, Tomsin K et al. Periodontal Disease and Pregnancy Outcomes: Overview of Systematic Reviews. JDR Clin Trans Res 2018;3(1):10-27.
- 19.Manrique-Corredor EJ, Orozco-Beltran D, Lopez-Pineda A et al. Maternal periodontitis and preterm birth: Systematic review and meta-analysis. Community Dent Oral Epidemiol 2019;47(3):243-51. doi: 10.1111/cdoe.12450.
- 20.Alnasser BH, Alkhaldi NK, Alghamdi WK, Alghamdi FT. The Potential Association Between Periodontal Diseases and Adverse Pregnancy Outcomes in Pregnant Women: A Systematic Review of Randomized Clinical Trials. Cureus 2023;15(1):e33216. doi: 10.7759/cureus.33216.
- 21.Le QA, Akhter R, Coulton KM et al. Periodontitis and Preeclampsia in Pregnancy: A Systematic Review and Meta-Analysis. Matern Child Health J 2022;26(12):2419-43. doi: 10.1007/s10995-022-03556-6.
- 22.Padilla-Cáceres T, Arbildo-Vega HI, Caballero-Apaza L et al. Association between the Risk of Preterm Birth and Low Birth Weight with Periodontal Disease in Pregnant Women: An Umbrella Review. Dent J (Basel) 2023;11(3):74. doi:10.3390/dj11030074.
- 23.Choi SE, Choudhary A, Ahern JM et al. Association between maternal periodontal disease and adverse pregnancy outcomes: an analysis of claims data. Fam Pract 2021;38:718-23. doi:10.1093/fampra/cmab037.
- 24.Teshome A, Yitayeh A. Relationship between periodontal disease and preterm low birth weight: systematic review. Pan Afr Med J 2016;24:215. doi:10.11604/pamj.2016.24.215.8727.
- 25.Butera A, Maiorani C, Morandini A et al. Periodontitis in Pregnant Women: A Possible Link to Adverse Pregnancy Outcomes. Healthcare (Basel) 2023;11(10):1372. doi:10.3390/healthcare11101372.
- 26.Parry S, Jeffcoat M, Reddy MS et al. Evaluation of an advanced oral hygiene regimen on maternity outcomes in a randomized multicenter clinical trial (Oral Hygiene and Maternity Outcomes Multicenter Study). Am J Obstet Gynecol MFM 2023;5:100995.
- 27.Patel N. The Impact of Periodontal Disease on Adverse Pregnancy Outcomes: A Comprehensive Review 21st World Congress in Fetal Medicine (Lisbon, Portugal; June, 2024).
- 28.American College of Obstetricians and Gynecologists. Oral Health Care During Pregnancy and Through the Lifespan. Committee Opinion, Number 569, August 2013. Reaffirmed 2025. https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2013/08/oral-health-care-during-pregnancy-and-through-the-lifespan.
- 29.Oral Health Care During Pregnancy Expert Workgroup. 2026. Oral Health Care During Pregnancy: A National Consensus Statement (rev. ed.). Washington, DC: National Maternal and Child Oral Health Resource Center. https://www.mchoralhealth.org/PDFs/OralHealthPregnancyConsensus.pdf#.
- 30.Bao J, Huang X, Wang L et al. Clinical practice guidelines for oral health care during pregnancy: a systematic evaluation and summary recommendations for general dental practitioners. Quintessence Int 2022;53(4):362-373. doi:10.3290/j.qi.b2644863.
- 31.American Dental Association. Pregnancy. https://www.ada.org/resources/ada-library/oral-health-topics/pregnancy.
- 32.American Dental Association. Radiographic Imaging, 2026. https://www.ada.org/resources/practice/practice-management/radiographic-imaging.
- 33.Anas M, Sultan MU, Fazal A. et al. Impact of periodontal therapy on adverse pregnancy outcomes: a systematic review of randomized controlled trials. Perio Implant Res 2025; 9:17. https://doi.org/10.1007/s41894-025-00161-y.
- 34.Iheozor-Ejiofor Z, Middleton P, Esposito M, Glenny AM. Treating periodontal disease for preventing adverse birth outcomes in pregnant women. Cochrane Database Syst Rev 2017;6:CD005297. doi:10.1002/14651858.CD005297.pub3.
- 35.Ramanauskaite E, Maciulskiene V, Baseviciene N, Anuzyte R. A Survey of Lithuanian Pregnant Women’s Knowledge about Periodontal Disease, Its Prevalence and Possible Influence on Pregnancy Outcomes. Medicina 2024;60:1431. https://doi.org/10.3390/medicina60091431.
- 36.Naavaal S, Brickhouse TH, Hafidh S, Smith K. Factors Associated with Preventive Dental Visits Before and During Pregnancy. J Womens Health (Larchmt) 2019;28(12):1670-8. doi:10.1089/jwh.2018.7509.
- 37.Texas Health and Human Services. Pregnancy Risk Assessment Monitoring System (PRAMS) Survey 2018 Data Book: Summary Tables. https://www.dshs.texas.gov/sites/default/files/mch/pdf/2018-PRAMS-Databook.pdf.
- 38.Chenwi H, Savitz D. Distribution of Preventive Dental Care during pregnancy in Rhode Island, 2012 to 2015. Rhode Island Medical Journal 2018:19-22. http://rimed.org/rimedicaljournal/2018/11/2018-11-19-cont-chenwi.pdf.
- 39.Azarshahri A, Rainchuso L, Vineyard J, Giblin-Scanlon L. Postpartum U.S. Women's Oral Health Knowledge, Attitudes, and Practices During Pregnancy. Matern Child Health J 2022;26(6):1339-49. doi:10.1007/s10995-021-03326-w.
- 40.Hoerler SB, Jenkins S, Assad D. Evaluating Oral Health in Pregnant Women: Knowledge, attitudes and practices of health professionals . J Dent Hyg 2019;93(1):16-22.
- 41.Rocha JS, Arima L, Chibinski AC et al. Barriers and facilitators to dental care during pregnancy: a systematic review and meta-synthesis of qualitative studies. Cad Saúde Pública 2018;34:e00130817. doi:10.1590/0102-311X00130817.
- 42.Kamalabadi YM, Campbell MK, Zitoun NM et al. Unfavourable beliefs about oral health and safety of dental care during pregnancy: a systematic review. BMC Oral Health 2023;23:762. https://doi.org/10.1186/s12903-023-03439-4.
- 43.George A, Johnson M, Duff M et al. Midwives and oral health care during pregnancy: perceptions of pregnant women in south-western Sydney, Australia. J Clin Nurs 2012;21(7-8):1087-96. doi:10.1111/j.1365-2702.2011.03870.x.
- 44.Ebinghaus M, Agricola CJ, Schmittinger J et al. Assessment of women's needs and wishes regarding interprofessional guidance on oral health in pregnancy - a qualitative study. BMC Pregnancy Childbirth 2024;24(1):471. doi:10.1186/s12884-024-06675-w.
- 45.Kamalabadi YM, Campbell MK, Gratton R et al. Oral health-related beliefs among a sample of pregnant women in Southwestern Ontario: a descriptive study. Front Oral Health 2024;5:1485815. doi:10.3389/froh.2024.1485815.
- 46.Al‐Swuailem AS. Knowledge of periodontal disease in expecting mothers and its association with utilization of dental services in Riyadh, Saudi Arabia. Pak Oral Dent J 2015;35(2):238-43.
- 47.Velosa‐Porras J, Rodríguez Malagón, N. Perceptions, knowledge, and practices related to oral health in a group of pregnant women: A qualitative study. Clin Exp Dent Res 2024;10:e823. https://doi.org/10.1002/cre2.823.
- 48.Rasubala L, Russell SL, Ren Y et al. Dental Faculty Knowledge, Attitudes, and Willingness to Treat Pregnant Persons at 2 Institutions. JDR Clin Trans Res 2025;10(Suppl 1):58S-66S. doi:10.1177/23800844251328637.
- 49.Huang SS, Yang C, Cohen V, Russell SL. What Factors Influence Dental Faculty's Willingness to Treat Pregnant Women? JDR Clin Trans Res 2022;7(4):407-14. doi: 10.1177/23800844211028132.
- 50.Schramm SA, Jacks ME, Prihoda TJ et al. Oral Care for Pregnant Patients: A Survey of Dental Hygienists' Knowledge, Attitudes and Practice. J Dent Hyg 2016;90(2):121-7.
- 51.Boutigny H, de Moegen M-L, Egea L et al. Oral Infections and Pregnancy: Knowledge of Gynecologists/Obstetricians, Midwives and Dentists. Oral Health Prev Dent 2016;14(1):41-7. doi:10.3290/j.ohpd.a34376.
- 52.AlHalal H, Albayyat R M, Alfhaed N K et al. Knowledge, Attitude, and Practice Regarding Periodontal and Dental Diseases During Pregnancy Among Obstetricians and Dentists in King Saud University Medical City. Cureus 2023;15(10): e47098. doi:10.7759/cureus.47098.
- 53.Naavaal S, Claiborne DM. Oral Health Knowledge, Practices, and Awareness of Oral Health Guidelines and Dental Coverage Policies among Midwives. J Midwifery Womens Health 2021;66(1):88-95. doi:10.1111/jmwh.13191.
- 54.George A, Ajwani S, Bhole S et al. Knowledge, attitude and practises of dentists towards oral health care during pregnancy: A cross sectional survey in New South Wales, Australia. Aust Dent J 2017;62(3):301-10. doi: 10.1111/adj.12505.
- 55.Skvoretz J, Dyer K, Daley E et al. Research and Practice Communications Between Oral Health Providers and Prenatal Health Providers: A Bibliometric Analysis. Matern Child Health J 2016 Aug;20(8):1607-19. doi: 10.1007/s10995-016-1960-x.
- 56.Bostanci N. Periodontal health and pregnancy outcomes: time to deliver. Acta Obstet Gynecol Scand 2023;102:648-51. 10.1111/aogs.14548.