

Gastroesophageal Reflux Disease: Implications and Management
Gastroesophageal Reflux Disease (GERD) has been defined as ‘a disease that is associated with troublesome symptoms and/or complications on account of reflux of stomach contents into the esophagus.’1Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R, Globale Konsensusgruppe. The Montreal definition and classification of gastroesophageal reflux disease: a global, evidence-based consensus paper. [Article in German] Z Gastroenterol 2007;45(11):1125-40. doi: 10.1055/s-2007-963633. The clinical presentation, signs and symptoms vary by patient as do complications of GERD, which is associated with dental erosion. Over the last 25 years, the prevalence of GERD has increased.2Burton L, Beattie J, Falk GL, Van der Wall H, Coman W. The burden of gastroesophageal reflux disease on the cost of managing chronic diseases in Australia. The need for a new diagnostic and management paradigm. Chronic Illn 2020;1742395320966373. doi: 10.1177/1742395320966373. Online ahead of print.,3El-Serag HB, Sweet S, Winchester CC, Dent J. Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut 2014;63(6):871-80. doi: 10.1136/gutjnl-2012-304269.,4Andreasson A, Talley NJ, Walker MM, Jones MP, Platts LG, Wallner B, et al. An Increasing Incidence of Upper Gastrointestinal Disorders Over 23 Years: A Prospective Population-Based Study in Sweden. Am J Gastroenterol 2020 Oct 7. Online ahead of print. doi: 10.14309/ajg.0000000000000972. It is now recognized as a global public health issue with a significant impact on health, quality of life and costs.2Burton L, Beattie J, Falk GL, Van der Wall H, Coman W. The burden of gastroesophageal reflux disease on the cost of managing chronic diseases in Australia. The need for a new diagnostic and management paradigm. Chronic Illn 2020;1742395320966373. doi: 10.1177/1742395320966373. Online ahead of print.,5Bert F, Pompili E, Lo Moro G, Corradi A, Sagrawa Caro A, Gualano MR, Siliquini R. Prevalence of gastro-esophageal reflux symptoms: an Italian cross-sectional survey focusing on knowledge and attitudes towards lifestyle and nutrition. Int J Clin Pract 2020;e13758. doi: 10.1111/ijcp.13758. Online ahead of print. Screening and management for GERD, as well as preventive care and interventions to prevent and manage related sequelae, can reduce the impact of this common condition.
Prevalence of GERD
In a systematic review and meta-analysis with more than 460,000 individuals 15 years-of-age and over, a global prevalence of 13.3% was found based on the criteria of at least weekly frequency of heartburn or regurgitation.6Eusebi LH, Ratnakumaran R, Yuan Y, Solaymani-Dodaran M, Bazzoli F, Ford AC. Global prevalence of, and risk factors for, gastro-oesophageal reflux symptoms: a meta-analysis. Gut 2018;67:430-40. Prevalence for North America, South America, Europe, the Middle East, Australia and East Asia, respectively, was 18.1%-27.8%, 23%, 8.8%-25.9%, 8.7%-33.1%,11.6% and 2.5%-7.8% in a systematic review with 31 studies.4Andreasson A, Talley NJ, Walker MM, Jones MP, Platts LG, Wallner B, et al. An Increasing Incidence of Upper Gastrointestinal Disorders Over 23 Years: A Prospective Population-Based Study in Sweden. Am J Gastroenterol 2020 Oct 7. Online ahead of print. doi: 10.14309/ajg.0000000000000972. In a recent study in Chile with more than one thousand individuals (median age 40 years), a prevalence of 44.8% was found.7Manterola C, Grande L, Bustos L, Otzen T. Prevalence of gastroesophageal reflux disease: a population-based cross-sectional study in southern Chile. Gastroenterol Rep (IF 2.960 ) Pub Date: 2020-02-19. doi: 10.1093/gastro/goaa002.
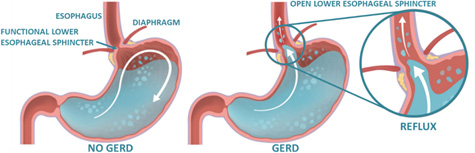
Figure 1. Role of the lower esophageal sphincter in GERD
Risk Factors and Etiology
GERD involves stomach contents, including gastric acid, moving through an open lower esophageal sphincter up into the esophagus. (Figure 1) This may be associated with reduced sphincter function, impaired function of the hiatus, or greater pressure in the stomach region.6Eusebi LH, Ratnakumaran R, Yuan Y, Solaymani-Dodaran M, Bazzoli F, Ford AC. Global prevalence of, and risk factors for, gastro-oesophageal reflux symptoms: a meta-analysis. Gut 2018;67:430-40. Risk factors include obesity and hiatus hernia (for which obesity is also a risk factor).8MacFarlane B. Management of gastroesophageal reflux disease in adults: a pharmacist's perspective. Integr Pharm Res Pract 2018;7:41-52. doi:10.2147/IPRP.S142932. ,9Argyrou A, Legaki E, Koutserimpas C, Gazouli M, Papaconstantinou I, Gkiokas G, Karamanolis G. Risk factors for gastroesophageal reflux disease and analysis of genetic contributors. World J Clin Cases 2018;6(8):176-82. doi:10.12998/wjcc.v6.i8.176. Central obesity changes the pressure gradient at the lower esophageal sphincter, while hiatus hernia loosens the sphincter, rendering it less effective as a barrier to reflux.8MacFarlane B. Management of gastroesophageal reflux disease in adults: a pharmacist's perspective. Integr Pharm Res Pract 2018;7:41-52. doi:10.2147/IPRP.S142932. ,9Argyrou A, Legaki E, Koutserimpas C, Gazouli M, Papaconstantinou I, Gkiokas G, Karamanolis G. Risk factors for gastroesophageal reflux disease and analysis of genetic contributors. World J Clin Cases 2018;6(8):176-82. doi:10.12998/wjcc.v6.i8.176. In addition, hiatus hernia and a high-fat diet are associated with increased GERD frequency and hiatus hernia with increased severity.8MacFarlane B. Management of gastroesophageal reflux disease in adults: a pharmacist's perspective. Integr Pharm Res Pract 2018;7:41-52. doi:10.2147/IPRP.S142932. Other risk factors include genetics, increasing age (50+ years), lifestyle, medications, eating shortly before bedtime (within 2 hours) and pregnancy.5Bert F, Pompili E, Lo Moro G, Corradi A, Sagrawa Caro A, Gualano MR, Siliquini R. Prevalence of gastro-esophageal reflux symptoms: an Italian cross-sectional survey focusing on knowledge and attitudes towards lifestyle and nutrition. Int J Clin Pract 2020;e13758. doi: 10.1111/ijcp.13758. Online ahead of print.,7Manterola C, Grande L, Bustos L, Otzen T. Prevalence of gastroesophageal reflux disease: a population-based cross-sectional study in southern Chile. Gastroenterol Rep (IF 2.960 ) Pub Date: 2020-02-19. doi: 10.1093/gastro/goaa002. ,8MacFarlane B. Management of gastroesophageal reflux disease in adults: a pharmacist's perspective. Integr Pharm Res Pract 2018;7:41-52. doi:10.2147/IPRP.S142932. ,9Argyrou A, Legaki E, Koutserimpas C, Gazouli M, Papaconstantinou I, Gkiokas G, Karamanolis G. Risk factors for gastroesophageal reflux disease and analysis of genetic contributors. World J Clin Cases 2018;6(8):176-82. doi:10.12998/wjcc.v6.i8.176.
The lower esophageal sphincter may have impaired resting tone or transient relaxations, permitting reflux. Relaxations frequency is reported to be affected by hormones, medications, dietary components and/or smoking.9Argyrou A, Legaki E, Koutserimpas C, Gazouli M, Papaconstantinou I, Gkiokas G, Karamanolis G. Risk factors for gastroesophageal reflux disease and analysis of genetic contributors. World J Clin Cases 2018;6(8):176-82. doi:10.12998/wjcc.v6.i8.176. Medications that are risk factors for GERD include, among others, nonsteroidal anti-inflammatory drugs, anticholinergics, estrogen replacement therapy, tricyclic antidepressants, statins, corticosteroids, benzodiazepines, calcium channel blockers and some antibiotics.8MacFarlane B. Management of gastroesophageal reflux disease in adults: a pharmacist's perspective. Integr Pharm Res Pract 2018;7:41-52. doi:10.2147/IPRP.S142932. ,9Argyrou A, Legaki E, Koutserimpas C, Gazouli M, Papaconstantinou I, Gkiokas G, Karamanolis G. Risk factors for gastroesophageal reflux disease and analysis of genetic contributors. World J Clin Cases 2018;6(8):176-82. doi:10.12998/wjcc.v6.i8.176. Consuming citrus or tomato products, chocolate, spicy foods, carbonated beverages, and alcohol consumption, may also be risk factors.8MacFarlane B. Management of gastroesophageal reflux disease in adults: a pharmacist's perspective. Integr Pharm Res Pract 2018;7:41-52. doi:10.2147/IPRP.S142932.
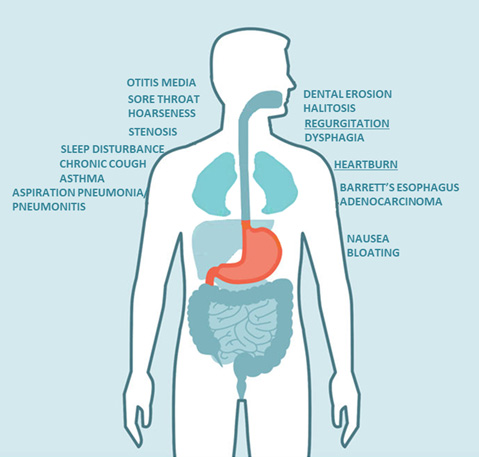
Figure 2. Signs, symptoms and complications of GERD
Signs and Symptoms
Clinically, GERD is categorized based on endoscopic findings as either erosive with injury to the esophageal mucosa or non-erosive. Symptoms typically include heartburn and regurgitation. Other potential (atypical) symptoms include sore throat, hoarseness, chronic cough, dysphagia, nausea, bloating, chest pain, otitis media, and stenosis of the laryngotracheal complex.7Manterola C, Grande L, Bustos L, Otzen T. Prevalence of gastroesophageal reflux disease: a population-based cross-sectional study in southern Chile. Gastroenterol Rep (IF 2.960 ) Pub Date: 2020-02-19. doi: 10.1093/gastro/goaa002. ,10Saracco M, Savarino V, Bodini G, Saracco GM, Pellicano R. Gastro-esophageal reflux disease: Key messages for clinicians. Minerva Gastroenterol Dietol 2020 Oct 26. Online ahead of print. doi: 10.23736/S1121-421X.20.02783-X.,11Seeras K, Bittar K, Siccardi MA. Nissen Fundoplication. [Updated 2020 Aug 25]. In: StatPearls [Internet]. StatPearls Publishing; 2020 Jan. Available at: https://www.ncbi.nlm.nih.gov/books/NBK519521/,12Lawrence L. Consider GERD in patients with pulmonary diseases. Pulmonology, March 2014. https://acpinternist.org/archives/2014/03/GERD.htm. Up to 25% of patients with GERD experience sleep disturbances and GERD may be linked to obstructive sleep apnea.13Shibli F, Skeans J, Yamasaki T, Fass R. Nocturnal gastroesophageal reflux disease (GERD) and sleep: An important relationship that Is commonly overlooked. J Clin Gastroenterol 2020;54(8):663-74. doi: 10.1097/MCG.0000000000001382. Additionally, GERD is one of the main risk factors for Barrett’s esophagus, a premalignancy in which the esophageal lining is altered and can lead to esophageal adenocarcinoma.6Eusebi LH, Ratnakumaran R, Yuan Y, Solaymani-Dodaran M, Bazzoli F, Ford AC. Global prevalence of, and risk factors for, gastro-oesophageal reflux symptoms: a meta-analysis. Gut 2018;67:430-40.,7Manterola C, Grande L, Bustos L, Otzen T. Prevalence of gastroesophageal reflux disease: a population-based cross-sectional study in southern Chile. Gastroenterol Rep (IF 2.960 ) Pub Date: 2020-02-19. doi: 10.1093/gastro/goaa002. ,14Uhlenhopp DJ, Then EO, Sunkara T, Gaduputi V. Epidemiology of esophageal cancer: update in global trends, etiology and risk factors. Clin J Gastroenterol 2020 Sep 23. Online ahead of print. doi: 10.1007/s12328-020-01237-x. Aspiration pneumonitis, which involves gastric acid aspirated into the lungs causing chemical damage, and aspiration pneumonia, are associated with GERD.2Burton L, Beattie J, Falk GL, Van der Wall H, Coman W. The burden of gastroesophageal reflux disease on the cost of managing chronic diseases in Australia. The need for a new diagnostic and management paradigm. Chronic Illn 2020;1742395320966373. doi: 10.1177/1742395320966373. Online ahead of print.,10Saracco M, Savarino V, Bodini G, Saracco GM, Pellicano R. Gastro-esophageal reflux disease: Key messages for clinicians. Minerva Gastroenterol Dietol 2020 Oct 26. Online ahead of print. doi: 10.23736/S1121-421X.20.02783-X. Chronic aspiration is associated with asthma, and GERD is linked to idiopathic pulmonary fibrosis. (Figure 2)
Dental Erosion (DE)
Figure 3. Moderate DE in a patient with GERD

Image of courtesy of Dr. Joyce Bassett
DE occurs following repeated exposure to extrinsic acids (e.g., low-pH beverages), or following exposure to intrinsic acid (gastric acid) due to reflux disease or repeated vomiting. This results in demineralization of the exposed dental surfaces, and erosive (mechanical) tooth wear of those surfaces by abrasion or attrition.15Picos A, Lasserre JF, Chisnoiu AM, Berar AM, d'Incau E, Picos AM, et al. Factors associated with dental erosions in gastroesophageal reflux disease: a cross-sectional study in patients with heartburn. Med Pharm Rep 2020;93(1):23-9. doi:10.15386/mpr-1332. (Figure 3) Further, buffering capacity has also been found to be reduced in patients with GERD.16Moazzez R, Bartlett D, Anggiansah A. Dental erosion, gastro-oesophageal reflux disease and saliva: how are they related? J Dent 2004;32(6):489-94. doi: 10.1016/j.jdent.2004.03.004. In a systematic review of 27 studies from 1980 through 2019, a more than four-fold and two-fold risk for DE was found, respectively, for objectively and subjectively measured GERD or symptoms of GERD.17Jordão HWT, Coleman HG, Kunzmann AT, McKenna G. The association between erosive toothwear and gastro-oesophageal reflux-related symptoms and disease: A systematic review and meta-analysis. J Dent 2020;95:103284. doi: 10.1016/j.jdent.2020.103284. In a second systematic review with 10 studies and more than seven thousand patients, the prevalence of DE in patients with and without GERD was 48.8% and 20.5%, respectively.18Picos A, Badea ME, Dumitrascu DL. Dental erosion in gastro-esophageal reflux disease. A systematic review. Clujul Med 2018;91(4):387-90. doi: 10.15386/cjmed-1017. In the only study evaluating children, DE occurred in 98% of children with GERD, compared to almost 40% of adults, while age was not a factor for patients without GERD. No relationship was found for GERD and DE in 4 of the 10 studies.19Farahmand F, Sabbaghian M, Ghodousi S, Seddighoraee N, Abbasi M. Gastroesophageal reflux disease and tooth erosion: a cross-sectional observational study. Gut Liver 2013;7:278-81. In another systematic review, a statistically significant association between GERD and DE was found in 7 of 16 studies.20Marsicano JA, de Moura-Grec PG, Bonato RCS, de Carvalho Sales-Peres M, Sales-Peres A, de Carvalho Sales-Peres SH. Gastroesophageal reflux, dental erosion, and halitosis in epidemiological surveys: a systematic review. Eur J Gastroenterol Hepatol 2013;25(2):135-41. doi: 10.1097/MEG.0b013e32835ae8f7. One of the difficulties in comparing studies on GERD and on DE has been the use of different criteria, indices and survey tools, and the presence of confounders and small sample sizes in some studies.7Manterola C, Grande L, Bustos L, Otzen T. Prevalence of gastroesophageal reflux disease: a population-based cross-sectional study in southern Chile. Gastroenterol Rep (IF 2.960 ) Pub Date: 2020-02-19. doi: 10.1093/gastro/goaa002. ,20Marsicano JA, de Moura-Grec PG, Bonato RCS, de Carvalho Sales-Peres M, Sales-Peres A, de Carvalho Sales-Peres SH. Gastroesophageal reflux, dental erosion, and halitosis in epidemiological surveys: a systematic review. Eur J Gastroenterol Hepatol 2013;25(2):135-41. doi: 10.1097/MEG.0b013e32835ae8f7.,21Lechien JR, Chiesa-Estomba CM, Calvo Henriquez C, Mouawad F, Ristagno C, Barillari MR, et al. Laryngopharyngeal reflux, gastroesophageal reflux and dental disorders: A systematic review. PLoS ONE 2020;15(8):e0237581. https://doi.org/10.1371/journal.pone.0237581.
In some studies, erosive lesions were most prevalent on the maxillary palatal and mandibular lingual surfaces, while in some studies the rate of damage was higher for upper than lower incisors, and on palatal surfaces.16Moazzez R, Bartlett D, Anggiansah A. Dental erosion, gastro-oesophageal reflux disease and saliva: how are they related? J Dent 2004;32(6):489-94. doi: 10.1016/j.jdent.2004.03.004.,18Picos A, Badea ME, Dumitrascu DL. Dental erosion in gastro-esophageal reflux disease. A systematic review. Clujul Med 2018;91(4):387-90. doi: 10.15386/cjmed-1017.,21Lechien JR, Chiesa-Estomba CM, Calvo Henriquez C, Mouawad F, Ristagno C, Barillari MR, et al. Laryngopharyngeal reflux, gastroesophageal reflux and dental disorders: A systematic review. PLoS ONE 2020;15(8):e0237581. https://doi.org/10.1371/journal.pone.0237581. All surfaces can be affected, and once dentin is exposed patients may experience dentinal hypersensitivity. Advanced DE, unhindered, can result in pulpal involvement.
Other Intra-oral Conditions
Four studies supported a relationship between GERD and dental caries in adults in one review, and in another report an increased risk of dental caries in children and adolescents was noted.20Marsicano JA, de Moura-Grec PG, Bonato RCS, de Carvalho Sales-Peres M, Sales-Peres A, de Carvalho Sales-Peres SH. Gastroesophageal reflux, dental erosion, and halitosis in epidemiological surveys: a systematic review. Eur J Gastroenterol Hepatol 2013;25(2):135-41. doi: 10.1097/MEG.0b013e32835ae8f7.,22Mantegazza C, Angiero F, Zuccotti GV. Oral manifestations of gastrointestinal diseases in children. Part 3: Ulcerative colitis and gastro-oesophageal reflux disease. Eur J Paediatr Dent 2016;17(3):248-50. However, in a separate study, no increase in dental caries was observed.23Watanabe M, Nakatani E, Yoshikawa H, Kanno T, Nariai Y, Yoshino A, et al. Oral soft tissue disorders are associated with gastroesophageal reflux disease: retrospective study. BMC Gastroenterol 2017;17(1):92. doi:10.1186/s12876-017-0650-5. Conflicting results were also found across 5 studies reporting on differences in gingival and periodontal disease prevalence in patients with and without GERD.20Marsicano JA, de Moura-Grec PG, Bonato RCS, de Carvalho Sales-Peres M, Sales-Peres A, de Carvalho Sales-Peres SH. Gastroesophageal reflux, dental erosion, and halitosis in epidemiological surveys: a systematic review. Eur J Gastroenterol Hepatol 2013;25(2):135-41. doi: 10.1097/MEG.0b013e32835ae8f7. In addition, while gingivitis was more prevalent in patients with GERD in a Japanese study, poorer oral hygiene was also observed and the most common oral compliant was dry mouth.22Mantegazza C, Angiero F, Zuccotti GV. Oral manifestations of gastrointestinal diseases in children. Part 3: Ulcerative colitis and gastro-oesophageal reflux disease. Eur J Paediatr Dent 2016;17(3):248-50. Other reported issues include ulceration of the oral mucosa, erythema of the oral mucosa, halitosis and taste disturbance.20Marsicano JA, de Moura-Grec PG, Bonato RCS, de Carvalho Sales-Peres M, Sales-Peres A, de Carvalho Sales-Peres SH. Gastroesophageal reflux, dental erosion, and halitosis in epidemiological surveys: a systematic review. Eur J Gastroenterol Hepatol 2013;25(2):135-41. doi: 10.1097/MEG.0b013e32835ae8f7.,24Raibrown A, Giblin LJ, Boyd LD, Perry K. Gastroesophageal Reflux Disease Symptom Screening in a Dental Setting. J Dent Hyg 2017;91:44-8.
Figure 4. Lifestyle modifications

Management of GERD
Options for the management of GERD include lifestyle modifications, medical and surgical treatment.11Seeras K, Bittar K, Siccardi MA. Nissen Fundoplication. [Updated 2020 Aug 25]. In: StatPearls [Internet]. StatPearls Publishing; 2020 Jan. Available at: https://www.ncbi.nlm.nih.gov/books/NBK519521/,13Shibli F, Skeans J, Yamasaki T, Fass R. Nocturnal gastroesophageal reflux disease (GERD) and sleep: An important relationship that Is commonly overlooked. J Clin Gastroenterol 2020;54(8):663-74. doi: 10.1097/MCG.0000000000001382. Depending on the individual, recommended lifestyle modifications include eating smaller meals and more than 2 hours before bedtime, avoiding trigger foods and alcohol, smoking cessation and weight loss. (Figure 4) The use of antacids helps to relieve GERD symptoms.7Manterola C, Grande L, Bustos L, Otzen T. Prevalence of gastroesophageal reflux disease: a population-based cross-sectional study in southern Chile. Gastroenterol Rep (IF 2.960 ) Pub Date: 2020-02-19. doi: 10.1093/gastro/goaa002. Medication options include Histamine-2 blockers (H2-blockers/H2-antagonists), protein-pump inhibitors (PPI) and sucralfate.11Seeras K, Bittar K, Siccardi MA. Nissen Fundoplication. [Updated 2020 Aug 25]. In: StatPearls [Internet]. StatPearls Publishing; 2020 Jan. Available at: https://www.ncbi.nlm.nih.gov/books/NBK519521/ H2-blockers prevent histamine-induced secretion of gastric acid (e.g., Pepcid; Zantac; Tagamet), while PPI block the enzyme (proton pump) that controls gastric acid production (e.g., omeprazole (Prilosec), lansoprazole (Prevacid) and esomeprazole (Nexium)).25Drugs.com H2 antagonists. https://www.drugs.com/drug-class/h2-antagonists.html. ,26Drugs.com. Protein pump inhibitors. https://www.drugs.com/drug-class/proton-pump-inhibitors.html Sucralfate (Calafate) creates an adhesive barrier coating over mucosal surfaces, protecting them against gastric acid.27Drugs.com. Sucralfate. https://www.drugs.com/mtm/sucralfate.html. As with all medications, their contraindications, side effects and drug interactions must be considered in recommendations and prescribing. Surgical options are invasive and less commonly used. They include laparoscopic anti-reflux surgeries (LARS) and hernial repair. Repositioning of the gastric fundus around the esophagus, known as fundoplication, provides for sphincter pressure.11Seeras K, Bittar K, Siccardi MA. Nissen Fundoplication. [Updated 2020 Aug 25]. In: StatPearls [Internet]. StatPearls Publishing; 2020 Jan. Available at: https://www.ncbi.nlm.nih.gov/books/NBK519521/,13Shibli F, Skeans J, Yamasaki T, Fass R. Nocturnal gastroesophageal reflux disease (GERD) and sleep: An important relationship that Is commonly overlooked. J Clin Gastroenterol 2020;54(8):663-74. doi: 10.1097/MCG.0000000000001382.
Preventing and Managing DE
DE is irreversible, initially almost imperceptible, and with progression to a moderate or advanced stage results in esthetic and functional impairment and requires invasive care.18Picos A, Badea ME, Dumitrascu DL. Dental erosion in gastro-esophageal reflux disease. A systematic review. Clujul Med 2018;91(4):387-90. doi: 10.15386/cjmed-1017. This highlights the need for prompt identification of at-risk patients and prevention and management of DE. For individuals with dietary habits causing exposure to extrinsic acids (low-pH beverages, snacks, candies and foods), whether or not contributing to DE in patients with GERD, dietary guidance should be provided on avoiding low-pH foods, beverages, snacks and candies.
Preventive and Restorative Care
Minimally invasive preventive care can be implemented to prevent DE or further DE. Frequent use of fluorides and high-concentration fluorides is protective against DE.28 It was also concluded in a systematic review that use of stannous fluoride agents offered better anti-erosive properties for enamel than sodium fluoride.29Teixeira L, Manarte-Monteiro P, Manso MC. Enamel lesions: Meta-analysis on effect of prophylactic/therapeutic agents in erosive tissue loss. J Dent Sci 2016;11(3):215-24. doi: 10.1016/j.jds.2016.03.008. Tin compounds are precipitated that can form a protective layer at the tooth surface, and also provide for occlusion of open dentinal tubules in patients experiencing dentinal hypersensitivity.28Magalhães AC, Wiegand A, Rios D, Buzalaf MAR, Lussi A. Fluoride in dental erosion. Monogr Oral Sci 2011;22:158-70. doi: 10.1159/000325167. ,30Hines D, Xu S, Stranick M, Lavender S, Pilch S, Zhang YP, et al. Effect of a stannous fluoride toothpaste on dentinal hypersensitivity: In vitro and clinical evaluation. J Am Dent Assoc 2019;150(4S):S47-S59. doi: JADA article For advanced erosion, bonded direct and/or indirect restorations are required to restore function and esthetics.
Patients should receive oral hygiene instruction, including proper brushing technique and use a soft or ultra-soft bristled brush, and advised not to brush shortly after experiencing reflux31American Dental Association. Erosive tooth wear. https://www.ada.org/en/member-center/oral-health-topics/erosive-tooth-wear. . Patients can also be advised to rinse with a glass of water containing one teaspoon of sodium bicarbonate (baking soda) to help with buffering and increase the intraoral pH following an episode of GERD.31American Dental Association. Erosive tooth wear. https://www.ada.org/en/member-center/oral-health-topics/erosive-tooth-wear. In addition, H2 blockers, sucralfate, and in some patients PPI, are associated with dry mouth.27,32Scully CBE C. Drug effects on salivary glands: dry mouth. Oral Dis 2003;9:165-76. doi:10.1034/j.1601-0825.2003.03967.x This needs to be considered in preventive and treatment recommendations for caries prevention in addition to DE for patients using these medications since salivary flow, clearance of acid and buffering capacity are reduced.
Other Considerations
For individuals with or suspected of having GERD or another medical condition causing DE, a medical referral should be provided. In a two-center study, a validated questionnaire was used to screen for GERD in dental hygiene clinics.24 It was concluded that such screening should be performed routinely by dental professionals and could help identify at-risk patients for referral to a medical facility for early intervention. Dental visits are also an opportunity to educate patients with GERD on lifestyle modifications that can reduce GERD. Advice on diet can also encourage a healthier diet that is low in fats and other dietary components associated with GERD. Conversely, it is also recommended that all patients in the medical setting with confirmed or suspected GERD be referred to a dentist for evaluation.
Conclusions
GERD is increasing in prevalence globally, with implications for systemic and oral health, as well as quality of life. Patients with GERD can be advised on lifestyle modifications and receive treatment. In addition, DE is a frequent occurrence in patients with GERD and preventable. It is recommended that medical professionals refer patients with GERD to a dental professional for an oral evaluation and that dental professionals screen patients for GERD and refer patients to medical professionals. With timely patient education and care, GERD can be managed to improve patient health and DE can be prevented and minimized.
References
- 1.Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R, Globale Konsensusgruppe. The Montreal definition and classification of gastroesophageal reflux disease: a global, evidence-based consensus paper. [Article in German] Z Gastroenterol 2007;45(11):1125-40. doi: 10.1055/s-2007-963633.
- 2.Burton L, Beattie J, Falk GL, Van der Wall H, Coman W. The burden of gastroesophageal reflux disease on the cost of managing chronic diseases in Australia. The need for a new diagnostic and management paradigm. Chronic Illn 2020;1742395320966373. doi: 10.1177/1742395320966373. Online ahead of print.
- 3.El-Serag HB, Sweet S, Winchester CC, Dent J. Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut 2014;63(6):871-80. doi: 10.1136/gutjnl-2012-304269.
- 4.Andreasson A, Talley NJ, Walker MM, Jones MP, Platts LG, Wallner B, et al. An Increasing Incidence of Upper Gastrointestinal Disorders Over 23 Years: A Prospective Population-Based Study in Sweden. Am J Gastroenterol 2020 Oct 7. Online ahead of print. doi: 10.14309/ajg.0000000000000972.
- 5.Bert F, Pompili E, Lo Moro G, Corradi A, Sagrawa Caro A, Gualano MR, Siliquini R. Prevalence of gastro-esophageal reflux symptoms: an Italian cross-sectional survey focusing on knowledge and attitudes towards lifestyle and nutrition. Int J Clin Pract 2020;e13758. doi: 10.1111/ijcp.13758. Online ahead of print.
- 6.Eusebi LH, Ratnakumaran R, Yuan Y, Solaymani-Dodaran M, Bazzoli F, Ford AC. Global prevalence of, and risk factors for, gastro-oesophageal reflux symptoms: a meta-analysis. Gut 2018;67:430-40.
- 7.Manterola C, Grande L, Bustos L, Otzen T. Prevalence of gastroesophageal reflux disease: a population-based cross-sectional study in southern Chile. Gastroenterol Rep (IF 2.960 ) Pub Date: 2020-02-19. doi: 10.1093/gastro/goaa002.
- 8.MacFarlane B. Management of gastroesophageal reflux disease in adults: a pharmacist's perspective. Integr Pharm Res Pract 2018;7:41-52. doi:10.2147/IPRP.S142932.
- 9.Argyrou A, Legaki E, Koutserimpas C, Gazouli M, Papaconstantinou I, Gkiokas G, Karamanolis G. Risk factors for gastroesophageal reflux disease and analysis of genetic contributors. World J Clin Cases 2018;6(8):176-82. doi:10.12998/wjcc.v6.i8.176.
- 10.Saracco M, Savarino V, Bodini G, Saracco GM, Pellicano R. Gastro-esophageal reflux disease: Key messages for clinicians. Minerva Gastroenterol Dietol 2020 Oct 26. Online ahead of print. doi: 10.23736/S1121-421X.20.02783-X.
- 11.Seeras K, Bittar K, Siccardi MA. Nissen Fundoplication. [Updated 2020 Aug 25]. In: StatPearls [Internet]. StatPearls Publishing; 2020 Jan. Available at: https://www.ncbi.nlm.nih.gov/books/NBK519521/
- 12.Lawrence L. Consider GERD in patients with pulmonary diseases. Pulmonology, March 2014. https://acpinternist.org/archives/2014/03/GERD.htm.
- 13.Shibli F, Skeans J, Yamasaki T, Fass R. Nocturnal gastroesophageal reflux disease (GERD) and sleep: An important relationship that Is commonly overlooked. J Clin Gastroenterol 2020;54(8):663-74. doi: 10.1097/MCG.0000000000001382.
- 14.Uhlenhopp DJ, Then EO, Sunkara T, Gaduputi V. Epidemiology of esophageal cancer: update in global trends, etiology and risk factors. Clin J Gastroenterol 2020 Sep 23. Online ahead of print. doi: 10.1007/s12328-020-01237-x.
- 15.Picos A, Lasserre JF, Chisnoiu AM, Berar AM, d'Incau E, Picos AM, et al. Factors associated with dental erosions in gastroesophageal reflux disease: a cross-sectional study in patients with heartburn. Med Pharm Rep 2020;93(1):23-9. doi:10.15386/mpr-1332.
- 16.Moazzez R, Bartlett D, Anggiansah A. Dental erosion, gastro-oesophageal reflux disease and saliva: how are they related? J Dent 2004;32(6):489-94. doi: 10.1016/j.jdent.2004.03.004.
- 17.Jordão HWT, Coleman HG, Kunzmann AT, McKenna G. The association between erosive toothwear and gastro-oesophageal reflux-related symptoms and disease: A systematic review and meta-analysis. J Dent 2020;95:103284. doi: 10.1016/j.jdent.2020.103284.
- 18.Picos A, Badea ME, Dumitrascu DL. Dental erosion in gastro-esophageal reflux disease. A systematic review. Clujul Med 2018;91(4):387-90. doi: 10.15386/cjmed-1017.
- 19.Farahmand F, Sabbaghian M, Ghodousi S, Seddighoraee N, Abbasi M. Gastroesophageal reflux disease and tooth erosion: a cross-sectional observational study. Gut Liver 2013;7:278-81.
- 20.Marsicano JA, de Moura-Grec PG, Bonato RCS, de Carvalho Sales-Peres M, Sales-Peres A, de Carvalho Sales-Peres SH. Gastroesophageal reflux, dental erosion, and halitosis in epidemiological surveys: a systematic review. Eur J Gastroenterol Hepatol 2013;25(2):135-41. doi: 10.1097/MEG.0b013e32835ae8f7.
- 21.Lechien JR, Chiesa-Estomba CM, Calvo Henriquez C, Mouawad F, Ristagno C, Barillari MR, et al. Laryngopharyngeal reflux, gastroesophageal reflux and dental disorders: A systematic review. PLoS ONE 2020;15(8):e0237581. https://doi.org/10.1371/journal.pone.0237581.
- 22.Mantegazza C, Angiero F, Zuccotti GV. Oral manifestations of gastrointestinal diseases in children. Part 3: Ulcerative colitis and gastro-oesophageal reflux disease. Eur J Paediatr Dent 2016;17(3):248-50.
- 23.Watanabe M, Nakatani E, Yoshikawa H, Kanno T, Nariai Y, Yoshino A, et al. Oral soft tissue disorders are associated with gastroesophageal reflux disease: retrospective study. BMC Gastroenterol 2017;17(1):92. doi:10.1186/s12876-017-0650-5.
- 24.Raibrown A, Giblin LJ, Boyd LD, Perry K. Gastroesophageal Reflux Disease Symptom Screening in a Dental Setting. J Dent Hyg 2017;91:44-8.
- 25.Drugs.com H2 antagonists. https://www.drugs.com/drug-class/h2-antagonists.html.
- 26.Drugs.com. Protein pump inhibitors. https://www.drugs.com/drug-class/proton-pump-inhibitors.html
- 27.Drugs.com. Sucralfate. https://www.drugs.com/mtm/sucralfate.html.
- 28.Magalhães AC, Wiegand A, Rios D, Buzalaf MAR, Lussi A. Fluoride in dental erosion. Monogr Oral Sci 2011;22:158-70. doi: 10.1159/000325167.
- 29.Teixeira L, Manarte-Monteiro P, Manso MC. Enamel lesions: Meta-analysis on effect of prophylactic/therapeutic agents in erosive tissue loss. J Dent Sci 2016;11(3):215-24. doi: 10.1016/j.jds.2016.03.008.
- 30.Hines D, Xu S, Stranick M, Lavender S, Pilch S, Zhang YP, et al. Effect of a stannous fluoride toothpaste on dentinal hypersensitivity: In vitro and clinical evaluation. J Am Dent Assoc 2019;150(4S):S47-S59. doi: JADA article
- 31.American Dental Association. Erosive tooth wear. https://www.ada.org/en/member-center/oral-health-topics/erosive-tooth-wear.
- 32.Scully CBE C. Drug effects on salivary glands: dry mouth. Oral Dis 2003;9:165-76. doi:10.1034/j.1601-0825.2003.03967.x