

Multiple Sclerosis and Oral Health
Multiple sclerosis (MS), a chronic auto-immune disease, affects an estimated one million individuals in the U.S. alone, with an estimated healthcare burden greater than $ 24 billion.1Tafti D, Ehsan M, Xixis KL. Multiple Sclerosis. StatPearls [Internet]. Last Update: September 7, 2022. https://www.ncbi.nlm.nih.gov/books/NBK499849/.,2Covello F, Ruoppolo G, Carissimo C et al. Multiple Sclerosis: Impact on Oral Hygiene, Dysphagia, and Quality of Life. Int J Environ Res Public Health 2020;17(11):3979. doi: 10.3390/ijerph17113979.,3John Hopkins. Multiple sclerosis. https://www.hopkinsmedicine.org/health/conditions-and-diseases/multiple-sclerosis-ms.,4Garg N, Smith TW. An update on immunopathogenesis, diagnosis, and treatment of multiple sclerosis. Brain Behav 2015;5(9):e00362. doi: 10.1002/brb3.362.,5National Multiple Sclerosis Society. Landmark Study Estimates Nearly 1 Million in the U.S. Have Multiple Sclerosis. February 15, 2019. Available at: https://www.nationalmssociety.org/About-the-Society/News/Landmark-Study-Estimates-Nearly%C2%A01-Million-in-the-U.,6ACROBiosystems. Multiple Sclerosis: Etiology, Pathology, Pathogenesis and Therapeutic Drugs. (2022). Available at: acrobio.com/A1571--Multiple-Sclerosis%3A-Etiology-Pathology-Pathogenesis-and-Therapeutic-Drugs.html?gclid=EAIaIQobChMIsK-clN2q_wIVshCtBh3NDQVKEAAYASAAEgITDPD_BwE. MS is more prevalent in females and can occur at any age, with onset usually between 20 and 40 years-of-age.2Covello F, Ruoppolo G, Carissimo C et al. Multiple Sclerosis: Impact on Oral Hygiene, Dysphagia, and Quality of Life. Int J Environ Res Public Health 2020;17(11):3979. doi: 10.3390/ijerph17113979.,7Mayo Clinic. Multiple sclerosis. https://www.mayoclinic.org/diseases-conditions/multiple-sclerosis/symptoms-causes/syc-20350269 In this article, we will review MS and its implications for oral health and treatment.
Types of MS
There are four main types of MS. For 70% to 80% of individuals, MS is ‘relapsing-remitting’ with symptoms that develop over a period of up to several weeks and last for 1 to 2 days, before partial or complete remission.1Tafti D, Ehsan M, Xixis KL. Multiple Sclerosis. StatPearls [Internet]. Last Update: September 7, 2022. https://www.ncbi.nlm.nih.gov/books/NBK499849/.,8Ghasemi N, Razavi S, Nikzad E. Multiple Sclerosis: Pathogenesis, Symptoms, Diagnoses and Cell-Based Therapy. Cell J 2017;19(1):1-10. doi: 10.22074/cellj.2016.4867. Twenty to 40% of these individuals will later develop ‘secondary progressive’ MS.7Mayo Clinic. Multiple sclerosis. https://www.mayoclinic.org/diseases-conditions/multiple-sclerosis/symptoms-causes/syc-20350269 The third type of MS is ‘progressive-relapsing’, and for 15% to 20% of patients MS is ‘primary progressive’ (no remissions). Ongoing disability is generally evident a decade or more after the first symptoms appear.1Tafti D, Ehsan M, Xixis KL. Multiple Sclerosis. StatPearls [Internet]. Last Update: September 7, 2022. https://www.ncbi.nlm.nih.gov/books/NBK499849/.,3John Hopkins. Multiple sclerosis. https://www.hopkinsmedicine.org/health/conditions-and-diseases/multiple-sclerosis-ms. In a few individuals, a single flare-up, severe MS with rapid progression, or a mild variant with ongoing progression but limited disability occurs.
Figure 1. Demyelination in multiple sclerosis
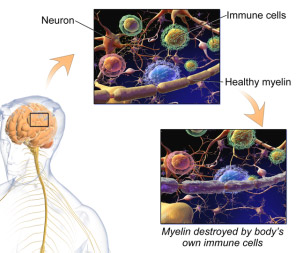
Source: BruceBlaus, CC BY-SA 4.0 https://creativecommons.org/licenses/by-sa/4.0, via Wikimedia Commons
The disease process
In MS, immune-mediated chronic inflammation causes destruction of the protective myelin sheath around the body’s nerve fibers (demyelination), creating localized scar tissue (plaques/sclerosis).3John Hopkins. Multiple sclerosis. https://www.hopkinsmedicine.org/health/conditions-and-diseases/multiple-sclerosis-ms. In addition, damage to the blood-brain barrier occurs as well as apoptosis of the oligodendrocytes that produce myelin for the central nervous system (CNS). Degeneration of neurons and axonal damage results in damage to the brain’s gray matter.3John Hopkins. Multiple sclerosis. https://www.hopkinsmedicine.org/health/conditions-and-diseases/multiple-sclerosis-ms.,6ACROBiosystems. Multiple Sclerosis: Etiology, Pathology, Pathogenesis and Therapeutic Drugs. (2022). Available at: acrobio.com/A1571--Multiple-Sclerosis%3A-Etiology-Pathology-Pathogenesis-and-Therapeutic-Drugs.html?gclid=EAIaIQobChMIsK-clN2q_wIVshCtBh3NDQVKEAAYASAAEgITDPD_BwE. (Figure 1) The immune response involves macrophages, T and B cells. Activated T cells enter the CNS, where they release pro-inflammatory cytokines.9National Multiple Sclerosis Society. https://www.nationalmssociety.org/What-is-MS/What-Causes-MS These cytokines include Interferon-γ, TNF-α, and IL-17,-21,-22,-26.8Ghasemi N, Razavi S, Nikzad E. Multiple Sclerosis: Pathogenesis, Symptoms, Diagnoses and Cell-Based Therapy. Cell J 2017;19(1):1-10. doi: 10.22074/cellj.2016.4867. B cells are also activated and produce antibodies and other proteins, damaging the CNS. In MS, anti-inflammatory T regulatory cells do not function normally.
Etiology
Environmental factors play a role in the etiology of MS and are believed to include a temperate climate (latitude), vitamin D deficiency, obesity (in females), and certain infectious agents.2Covello F, Ruoppolo G, Carissimo C et al. Multiple Sclerosis: Impact on Oral Hygiene, Dysphagia, and Quality of Life. Int J Environ Res Public Health 2020;17(11):3979. doi: 10.3390/ijerph17113979.,37Hajeer S, Nasr F, Nabha S et al. Association between vitamin D deficiency and multiple sclerosis- MRI significance: A scoping review. Heliyon 2023;9(5):e15754. doi: 10.1016/j.heliyon.2023.e15754.,10Simpson S, Blizzard L, Otahal P et al. Latitude is significantly associated with the prevalence of multiple sclerosis: a meta-analysis. J Neurol Neurosurg Psychiatry 2011;82(10):1132-41.,11Sintzel MB, Rametta M, Reder AT. Vitamin D and Multiple Sclerosis: A Comprehensive Review. Neurol Ther 2018;7(1):59-85. Previous infection with the Epstein Barr virus (EBV) was found to likely be a contributing factor to the development of MS.7Mayo Clinic. Multiple sclerosis. https://www.mayoclinic.org/diseases-conditions/multiple-sclerosis/symptoms-causes/syc-20350269,9National Multiple Sclerosis Society. https://www.nationalmssociety.org/What-is-MS/What-Causes-MS Recently, a study has confirmed that EBV triggers MS by dysregulating the immune system.12Leggett H. How Epstein-Barr virus triggers multiple sclerosis Study identifies how Epstein-Barr virus triggers multiple sclerosis. Stanford Medicine News, January 24, 2022. https://med.stanford.edu/news/all-news/2022/01/epstein-barr-virus-multiple-sclerosis.html#:~:text=Previous%20research%20has%20shown%20that%20multiple%20sclerosis%20patients,prior%20infection%2C%20compared%20with%2094%25%20of%20healthy%20individuals.,13Lanz TV, Brewer RC, Ho PP et al. Clonally expanded B cells in multiple sclerosis bind EBV EBNA1 and GlialCAM. Nature 2022;603:321-7. https://doi.org/10.1038/s41586-022-04432-7 GlialCAM is found in myelin and made in the CNS, and since part of the EBV protein (EBNA1) mimics GlialCAM this results in both EBV and GlialCAM being attacked by the immune system. B cells from spinal fluid produce oligoclonal antibodies (antibody proteins) that are part of an MS diagnosis. These antibodies bind to EBNA1 and to GlialCAM. The same area of EBNA1 was identified in a prior study in which 800 of 801 individuals with MS were EBV-positive. The latest study has produced strong evidence that in the overwhelming majority of cases MS is triggered by EBV.
Figure 2. Main symptoms of MS
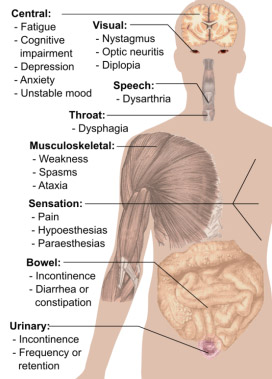
Image courtesy of Mikael Häggström
Genetic factors influence susceptibility to MS.2Covello F, Ruoppolo G, Carissimo C et al. Multiple Sclerosis: Impact on Oral Hygiene, Dysphagia, and Quality of Life. Int J Environ Res Public Health 2020;17(11):3979. doi: 10.3390/ijerph17113979.,3John Hopkins. Multiple sclerosis. https://www.hopkinsmedicine.org/health/conditions-and-diseases/multiple-sclerosis-ms.,9National Multiple Sclerosis Society. https://www.nationalmssociety.org/What-is-MS/What-Causes-MS Among individuals in the Swedish Registry, when a monozygotic or dizygotic twin had MS, a 23-fold and 2-fold risk of MS, respectively, was found for the other twin compared to the general population.14Westerlind H, Ramanujam R, Uvehag D et al. Modest familial risks for multiple sclerosis: a registry-based study of the population of Sweden. Brain 2014;137(Pt 3):770-8. doi: 10.1093/brain/awt356. For children of a parent with MS, a more than five-fold risk was found. Genetic predisposition is associated with certain human leukocyte antigen (HLA) haplotypes.15Cavallo S. Immune-mediated genesis of multiple sclerosis. J Transl Autoimmun 2020;3:100039. doi: 10.1016/j.jtauto.2020.100039. In particular, HLA DRB1*1501 strongly correlates with MS.9National Multiple Sclerosis Society. https://www.nationalmssociety.org/What-is-MS/What-Causes-MS,16Alcina A, Abad-Grau M, Fedetz M et al. Multiple sclerosis risk variant HLA-DRB1*1501 associates with high expression of DRB1 gene in different human populations. PLoS One 2012;7(1):e29819. A slightly elevated risk for MS is present in individuals with other autoimmune diseases (e.g., psoriasis, inflammatory bowel disease).7Mayo Clinic. Multiple sclerosis. https://www.mayoclinic.org/diseases-conditions/multiple-sclerosis/symptoms-causes/syc-20350269 Additionally, along with shared genetic features, psoriasis has been found to elevate risk for MS, independent of other autoimmune diseases considered.17Patrick MT, Nair RP, He K et al. Shared Genetic Risk Factors for Multiple Sclerosis/Psoriasis Suggest Involvement of Interleukin-17 and Janus Kinase-Signal Transducers and Activators of Transcription Signaling. Ann Neurol 2023 May 1. doi: 10.1002/ana.26672.
Signs and symptoms of MS
Typical initial symptoms include blurred/double vision, unilateral loss of vision (partial or complete), ocular pain, difficulty walking, paresthesia, and tingling or numbness in one area.8Ghasemi N, Razavi S, Nikzad E. Multiple Sclerosis: Pathogenesis, Symptoms, Diagnoses and Cell-Based Therapy. Cell J 2017;19(1):1-10. doi: 10.22074/cellj.2016.4867. MS symptoms also include fatigue, optic neuritis, numbness/weakness in a limb, unsteady gait, poor coordination, paralysis, slurred speech, dysphagia, hearing loss, vertigo, sexual dysfunction, bowel and bladder incontinence, poor cognition and mood disturbance.3John Hopkins. Multiple sclerosis. https://www.hopkinsmedicine.org/health/conditions-and-diseases/multiple-sclerosis-ms.,7Mayo Clinic. Multiple sclerosis. https://www.mayoclinic.org/diseases-conditions/multiple-sclerosis/symptoms-causes/syc-20350269,18Gür E, Binkhamis G, Kluk K. Effects of multiple sclerosis on the audio-vestibular system: a systematic review. BMJ Open 2022;12(8):e060540. doi: 10.1136/bmjopen-2021-060540. Resulting complications can include further muscle weakness, decreased bone density due to inactivity, repeated urinary tract infections, and pneumonia associated with dysphagia. Stress, anxiety and depression are common.3John Hopkins. Multiple sclerosis. https://www.hopkinsmedicine.org/health/conditions-and-diseases/multiple-sclerosis-ms. (Figure 2) Symptoms experienced by an individual depend on lesion location, the type of MS and its duration.
Oral complaints in patients with MS
Figure 3. Occurrence of orofacial manifestations in patients with MS19Danesh-Sani SA, Rahimdoost A, Soltani M et al. Clinical assessment of orofacial manifestations in 500 patients with multiple sclerosis. J Oral Maxillofac Surg 2013;71(2):290-4. doi: 10.1016/j.joms.2012.05.008.
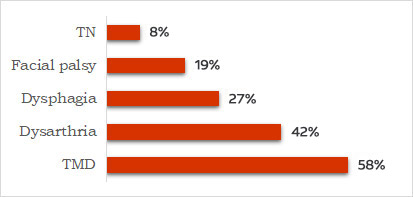
Figure 4. Oral complaints25Sexton C, Lalloo R, Stormon N et al. Oral health and behaviours of people living with Multiple Sclerosis in Australia. Community Dent Oral Epidemiol 2019;47:201-9.
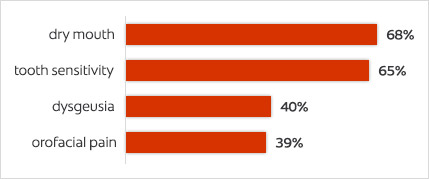
In a study with 500 patients (ages 11 to 69 years), 88.6% of patients with MS presented with orofacial involvement.19Danesh-Sani SA, Rahimdoost A, Soltani M et al. Clinical assessment of orofacial manifestations in 500 patients with multiple sclerosis. J Oral Maxillofac Surg 2013;71(2):290-4. doi: 10.1016/j.joms.2012.05.008. The most common manifestations were ocular, while temporomandibular disorders, dysarthria, dysphagia, facial palsy, and trigeminal neuralgia (TN) were observed in 58%, 42%, 27%, 19% and 8% of patients, respectively. Orofacial involvement was more common for patients with MS for more than 7 years. (Figure 3) TN, trigeminal sensory neuropathy, numbness, paresthesia, glossopharyngeal neuralgia and facial palsy are all manifestations of MS, and facial paralysis affects up to 24.3% of individuals.2Covello F, Ruoppolo G, Carissimo C et al. Multiple Sclerosis: Impact on Oral Hygiene, Dysphagia, and Quality of Life. Int J Environ Res Public Health 2020;17(11):3979. doi: 10.3390/ijerph17113979.,20Chemaly D, Lefrançois A, Pérusse R. Oral and maxillofacial manifestations of multiple sclerosis. J Can Dent Assoc 2000;66(11):600-5.,21Hooge JP, Redekop WK. Trigeminal neuralgia in multiple sclerosis. Neurol 1995;45:1294-6.,22Fukazawa T, Moriwaka F, Hamada K et al. Facial palsy in multiple sclerosis. J Neurol 1997;244:631-3. In addition, for patients experiencing TN, touch, mastication and brushing can trigger sharp pain of sudden onset.21Hooge JP, Redekop WK. Trigeminal neuralgia in multiple sclerosis. Neurol 1995;45:1294-6. Dysphagia was reported in other studies by 34%23Calcagno P, Ruoppolo G, Grasso MG et al. Dysphagia in multiple sclerosis—Prevalence and prognostic factors. Acta Neurol Scand 2002;105:40-3. doi: 10.1034/j.1600-0404.2002.10062.x. and 22%2Covello F, Ruoppolo G, Carissimo C et al. Multiple Sclerosis: Impact on Oral Hygiene, Dysphagia, and Quality of Life. Int J Environ Res Public Health 2020;17(11):3979. doi: 10.3390/ijerph17113979. of individuals with MS, and dysarthria by 38%.2Covello F, Ruoppolo G, Carissimo C et al. Multiple Sclerosis: Impact on Oral Hygiene, Dysphagia, and Quality of Life. Int J Environ Res Public Health 2020;17(11):3979. doi: 10.3390/ijerph17113979. Temporomandibular joint sounds and pain on opening are found to be more common in patients with MS than a control group in other research.24Kovac Z, Uhac I, Buković D et al. Oral health status and temporomandibular disorders in multiple sclerosis patients. Coll Antropol 2005;29(2):441-4. In a recent survey of more than fifteen hundred individuals with MS, 57% reported toothache in the prior year, more than three times the level in the general population.25Sexton C, Lalloo R, Stormon N et al. Oral health and behaviours of people living with Multiple Sclerosis in Australia. Community Dent Oral Epidemiol 2019;47:201-9. In addition, 68%, 65%, 40% and 39%, respectively, reported dry mouth, tooth sensitivity, dysgeusia and orofacial pain. (Figure 4) Other complaints include tremors, muscle weakness, and unilateral muscle spasms and contractions that can occur several times daily when the region’s motor nerves are affected.
MS Management
While MS is incurable, an early diagnosis enables early treatment.3John Hopkins. Multiple sclerosis. https://www.hopkinsmedicine.org/health/conditions-and-diseases/multiple-sclerosis-ms. The overall goal of treatment is to slow development and progression of the disease. For patients with relapsing-remitting MS, disease modifying medications are the primary method of treatment.3John Hopkins. Multiple sclerosis. https://www.hopkinsmedicine.org/health/conditions-and-diseases/multiple-sclerosis-ms.,26https://www.webmd.com/multiple-sclerosis/ms-treatment These include glatiramer acetate (Copaxone, Glatopa), dimethyl fumarate (Tecfidera), fingolimod (Gilenya), interferon-beta preparations, natalizumab (Tysabri), diroximel fumarate (Vumerity), mitoxantrone, rituximab (Rituxan), ofatumumab (Arzerra, Kesimpta), and ocrelizumab (Ocrevus). Disease-modifying medications are ineffective for progressive MS. A limited number of medications is also available to treat progressive types of MS. In addition, patients with MS require treatment to prevent or treat complications (e.g., vertigo, depression). Corticosteroids (e.g., methylprednisolone) are anti-inflammatory and immunomodulatory effects, and typically used during an acute relapse to ease symptoms and encourage recovery.4Garg N, Smith TW. An update on immunopathogenesis, diagnosis, and treatment of multiple sclerosis. Brain Behav 2015;5(9):e00362. doi: 10.1002/brb3.362. Given the wide array of medications used to treat MS and its complications, it is beyond the scope of this article to include all of them.
progression of the disease.
Medications and oral adverse events
Medications that suppress or modulate the immune system result in a lower resistance to systemic and oral infections, and immunosuppression of long-duration increases risk for lymphoma and oral squamous cell carcinoma.27College of dental hygienists of Ontario. Multiple sclerosis. https://www.cda-adc.ca/jcda/vol-66/issue-11/600.pdf. Intraorally, lowered resistance to infection results in an increased risk of oral infections, including candida (thrush and angular cheilitis).28Cockburn N, Pateman K, Taing MW et al. Managing the oral side effects of medications used to treat multiple sclerosis. Aust Dent J 2017;62:331-6. Oral adverse events for medications used to treat MS variously include dry mouth, oral ulcerations, burning mouth, dysgeusia, dysphagia, bleeding gums, oropharyngeal pain, circumoral paresthesia, oral swelling, cold sores, stomatitis, mucositis and salivary gland enlargement.26https://www.webmd.com/multiple-sclerosis/ms-treatment,27College of dental hygienists of Ontario. Multiple sclerosis. https://www.cda-adc.ca/jcda/vol-66/issue-11/600.pdf.,28Cockburn N, Pateman K, Taing MW et al. Managing the oral side effects of medications used to treat multiple sclerosis. Aust Dent J 2017;62:331-6.,29www.drugs.com (Table 1)
Table 1. MS medications and oral adverse events
| Medication | Reported oral adverse events |
|---|---|
| Alemtuzumab | Dysgeusia, oropharyngeal pain, oral herpes |
| Corticosteroids | Oral candidiasis, other oral infections |
| Glatiramer acetate | Dysphagia, dry mouth, burning mouth, stomatitis, oral ulcerations, bleeding gums, circumoral paresthesia, oral swelling, tongue discoloration, salivary gland enlargement |
| Interferon beta 1a | Dry mouth, oral ulcerations, bleeding gums, oral swelling, cold sores |
| Methotrexate | Gingivitis, oral ulcerations, mucositis |
| Mitrozantrone | Stomatitis, mucositis |
| Natalizumab | Stomatitis, oral ulcerations, tooth infections |
| Ocrelizumab | Cold sores |
| Teriflunomide | Toothache, dysgeusia |
For medications used to manage symptoms of MS, the most common adverse event is dry mouth. Such medications include antidepressants, anxiolytics, anti-convulsants, muscle relaxants, anti-spasmodics, and medications used to treat bladder dysfunctions, fatigue, impaired walking, urticaria and dizziness/vertigo.8Ghasemi N, Razavi S, Nikzad E. Multiple Sclerosis: Pathogenesis, Symptoms, Diagnoses and Cell-Based Therapy. Cell J 2017;19(1):1-10. doi: 10.22074/cellj.2016.4867. Other potential oral adverse events of anti-convulsants include oral ulcerations, dysphagia, erythema multiforme, glossitis, and dysgeusia. Hypersalivation is caused by anti-convulsants and anxiolytics, and gingival hyperplasia may result from use of phenytoin for pain management.27College of dental hygienists of Ontario. Multiple sclerosis. https://www.cda-adc.ca/jcda/vol-66/issue-11/600.pdf.
Implications for oral health and dental treatment
Individuals with MS are at risk for poor oral health, due to both MS and medication-related adverse events. Furthermore, the ability and willingness to perform oral hygiene is compromised by fatigue, a weak hand grip, muscle spasms, problems with coordination and, in some cases, compromised cognition and depression.30Multiple Sclerosis Society (MS Society UK). How can MS symptoms affect oral health? https://www.mssociety.org.uk/about-ms/signs-and-symptoms/oral-health.,31https://penndentalmedicine.org/patient-information/dentist-for-special-needs/multiple-sclerosis-and-dentist/,32Costa C, Santiago H, Pereira S et al. Oral Health Status and Multiple Sclerosis: Classic and Non-Classic Manifestations—Case Report. Diseases 2022;10:62. https:// doi.org/10.3390/diseases10030062./,33National Multiple Sclerosis Society. Dental Health. https://www.nationalmssociety.org/nationalmssociety/media/msnationalfiles/brochures/brochure-dental-health.pdf/ More frequent dental visits are indicated, and it is essential to thoroughly review medical records and to ask patients if anything has changed since their last visit.
Dental visits should generally be short, with breaks if needed, and scheduled in the morning when patients experience less fatigue.27College of dental hygienists of Ontario. Multiple sclerosis. https://www.cda-adc.ca/jcda/vol-66/issue-11/600.pdf.,33National Multiple Sclerosis Society. Dental Health. https://www.nationalmssociety.org/nationalmssociety/media/msnationalfiles/brochures/brochure-dental-health.pdf/ Patients may tire during dental treatment and have difficulty sitting still/keeping their mouths open due to muscle spasms, pain or numbness. Asking patients ahead about potential problems helps in finding solutions. For example, agreeing on a signal in case the patient needs you to stop while receiving treatment, adjusting your communication method, using mouth props, or reclining the dental chair only slightly to help avoid breathing difficulties.27College of dental hygienists of Ontario. Multiple sclerosis. https://www.cda-adc.ca/jcda/vol-66/issue-11/600.pdf.,31https://penndentalmedicine.org/patient-information/dentist-for-special-needs/multiple-sclerosis-and-dentist/ An individual may also need to accompany the patient to help them move, or reclining a wheelchair might work during treatment.
Significant and life-threatening adverse events may occur with specific medications,34WebMD. Drugs & Medications A–Z. Available at: webmd.com/drugs/indexdrugs. aspx. including a risk of these occurring during dental treatment. To determine potential contraindications, warnings, adverse events and drug interactions, the manufacturer’s full drug information should be consulted.
Advice and oral hygiene recommendations
Patients should be counselled on the oral effects of MS and their medications and provided with dietary and lifestyle advice. This includes providing information on smoking cessation to smokers since after an initial episode of MS they are more likely to experience further episodes than non-smokers.7Mayo Clinic. Multiple sclerosis. https://www.mayoclinic.org/diseases-conditions/multiple-sclerosis/symptoms-causes/syc-20350269 Dental professionals should also be aware that in patients with unexplained unilateral or bilateral orofacial paresthesia that this may be the initial manifestation of MS, be alert to this possibility and refer patients promptly to a physician.35Gallud L, Bagan JV, Cervelló A et al. Multiple sclerosis as first manifestation in oral and facial area: Presentation of four cases. Med Oral Patol Oral Cir Bucal 2006 ;11(2):E141-5.
Recommendations for oral hygiene for patients with MS include the following:
- Manual toothbrushes with bulky handles or looped handles to help improve grip and control of the brush.
- Power brushes with wide handles, requiring less grip and effort and automate movement of the brush head.
- Power brushes with apps can help guide brushing and motivate the user.
- If a patient has hand tremors, a weighted glove helps prevent hand shaking. Interdental cleaning may be easier with a home use irrigation device than with dental floss.
- Patients who tire easily can be advised to sit while brushing, and to perform interdental cleaning in the morning when they typically are less fatigued.33National Multiple Sclerosis Society. Dental Health. https://www.nationalmssociety.org/nationalmssociety/media/msnationalfiles/brochures/brochure-dental-health.pdf/
If necessary, individuals can seek help from another person for oral hygiene needs.
Preventing and managing oral disease
Dry mouth places individuals at elevated risk for dental caries, dental erosion, and other complications. For caries control, recommendations include in-office application of 5% sodium fluoride varnish as well as home use of a prescription-level 5000 ppm fluoride toothpaste.36Weyant RJ, Tracy SL, Anselmo TT et al; American Dental Association Council on Scientific Affairs Expert Panel on Topical Fluoride Caries Preventive Agents. Topical fluoride for caries prevention: executive summary of the updated clinical recommendations and supporting systematic review. J Am Dent Assoc 2013;144(11):1279-91. doi: 10.14219/jada.archive.2013.0057. In addition, silver diamine fluoride can be applied in-office to caries lesions. Prompt intervention with fluorides helps to prevent incipient lesions and to arrest and reverse existing lesions. Fluorides are also protective against dental erosion. Patients can be advised on the use of salivary substitutes, and other methods to relieve dry mouth and, as necessary, provided with advice and treatment indicated by other oral conditions that may occur. Patients with oral infections will require treatment, such as antifungal therapy for candidal infections. For oral ulcerations, irritations and other conditions palliative care can be provided.
Other considerations
In a scoping review (2023), in several studies fewer and lower-volume MRI-detected lesions were found with vitamin D supplementation, an alternative therapy that has been recommended for patients with MS.37Hajeer S, Nasr F, Nabha S et al. Association between vitamin D deficiency and multiple sclerosis- MRI significance: A scoping review. Heliyon 2023;9(5):e15754. doi: 10.1016/j.heliyon.2023.e15754. For the management of symptoms, acupuncture, cooling treatments, exercise, a healthy diet, cognitive therapy and stress management have been suggested.38Complementary and Alternative Medicines and Multiple Sclerosis. https://www.nationalmssociety.org/Treating-MS/Complementary-Alternative-Medicines.
Recent research confirming the role of EBV in MS suggests that a vaccine could prevent MS and vaccines using RNA technology or DNA plasmids and is considered promising.12Leggett H. How Epstein-Barr virus triggers multiple sclerosis Study identifies how Epstein-Barr virus triggers multiple sclerosis. Stanford Medicine News, January 24, 2022. https://med.stanford.edu/news/all-news/2022/01/epstein-barr-virus-multiple-sclerosis.html#:~:text=Previous%20research%20has%20shown%20that%20multiple%20sclerosis%20patients,prior%20infection%2C%20compared%20with%2094%25%20of%20healthy%20individuals. It is also suggested that in the future it may be possible to provide inoculations (treatment) for patients who already have MS, that could halt the autoimmune inflammatory process.
Conclusions
MS is a chronic debilitating disease impacting systemic and oral health, which are also impacted by the potential adverse events of medications used to treat MS and its symptoms. Dental professionals should be aware of the signs and symptoms of MS, including orofacial changes that may be an alert for a patient potentially developing MS, and the impact on oral health. Knowledge of the medications that patients are taking, and their potential adverse events, warnings and drug interactions is essential to providing dental treatment. It is necessary to obtain a full medical history for all patients (including medications and any alternative therapies they are receiving), to support and motivate patients’ oral hygiene efforts and attendance for dental visits, and to tailor interventions. Patient management requires an interdisciplinary approach.
References
- 1.Tafti D, Ehsan M, Xixis KL. Multiple Sclerosis. StatPearls [Internet]. Last Update: September 7, 2022. https://www.ncbi.nlm.nih.gov/books/NBK499849/.
- 2.Covello F, Ruoppolo G, Carissimo C et al. Multiple Sclerosis: Impact on Oral Hygiene, Dysphagia, and Quality of Life. Int J Environ Res Public Health 2020;17(11):3979. doi: 10.3390/ijerph17113979.
- 3.John Hopkins. Multiple sclerosis. https://www.hopkinsmedicine.org/health/conditions-and-diseases/multiple-sclerosis-ms.
- 4.Garg N, Smith TW. An update on immunopathogenesis, diagnosis, and treatment of multiple sclerosis. Brain Behav 2015;5(9):e00362. doi: 10.1002/brb3.362.
- 5.National Multiple Sclerosis Society. Landmark Study Estimates Nearly 1 Million in the U.S. Have Multiple Sclerosis. February 15, 2019. Available at: https://www.nationalmssociety.org/About-the-Society/News/Landmark-Study-Estimates-Nearly%C2%A01-Million-in-the-U.
- 6.ACROBiosystems. Multiple Sclerosis: Etiology, Pathology, Pathogenesis and Therapeutic Drugs. (2022). Available at: acrobio.com/A1571--Multiple-Sclerosis%3A-Etiology-Pathology-Pathogenesis-and-Therapeutic-Drugs.html?gclid=EAIaIQobChMIsK-clN2q_wIVshCtBh3NDQVKEAAYASAAEgITDPD_BwE.
- 7.Mayo Clinic. Multiple sclerosis. https://www.mayoclinic.org/diseases-conditions/multiple-sclerosis/symptoms-causes/syc-20350269
- 8.Ghasemi N, Razavi S, Nikzad E. Multiple Sclerosis: Pathogenesis, Symptoms, Diagnoses and Cell-Based Therapy. Cell J 2017;19(1):1-10. doi: 10.22074/cellj.2016.4867.
- 9.National Multiple Sclerosis Society. https://www.nationalmssociety.org/What-is-MS/What-Causes-MS
- 10.Simpson S, Blizzard L, Otahal P et al. Latitude is significantly associated with the prevalence of multiple sclerosis: a meta-analysis. J Neurol Neurosurg Psychiatry 2011;82(10):1132-41.
- 11.Sintzel MB, Rametta M, Reder AT. Vitamin D and Multiple Sclerosis: A Comprehensive Review. Neurol Ther 2018;7(1):59-85.
- 12.Leggett H. How Epstein-Barr virus triggers multiple sclerosis Study identifies how Epstein-Barr virus triggers multiple sclerosis. Stanford Medicine News, January 24, 2022. https://med.stanford.edu/news/all-news/2022/01/epstein-barr-virus-multiple-sclerosis.html#:~:text=Previous%20research%20has%20shown%20that%20multiple%20sclerosis%20patients,prior%20infection%2C%20compared%20with%2094%25%20of%20healthy%20individuals.
- 13.Lanz TV, Brewer RC, Ho PP et al. Clonally expanded B cells in multiple sclerosis bind EBV EBNA1 and GlialCAM. Nature 2022;603:321-7. https://doi.org/10.1038/s41586-022-04432-7
- 14.Westerlind H, Ramanujam R, Uvehag D et al. Modest familial risks for multiple sclerosis: a registry-based study of the population of Sweden. Brain 2014;137(Pt 3):770-8. doi: 10.1093/brain/awt356.
- 15.Cavallo S. Immune-mediated genesis of multiple sclerosis. J Transl Autoimmun 2020;3:100039. doi: 10.1016/j.jtauto.2020.100039.
- 16.Alcina A, Abad-Grau M, Fedetz M et al. Multiple sclerosis risk variant HLA-DRB1*1501 associates with high expression of DRB1 gene in different human populations. PLoS One 2012;7(1):e29819.
- 17.Patrick MT, Nair RP, He K et al. Shared Genetic Risk Factors for Multiple Sclerosis/Psoriasis Suggest Involvement of Interleukin-17 and Janus Kinase-Signal Transducers and Activators of Transcription Signaling. Ann Neurol 2023 May 1. doi: 10.1002/ana.26672.
- 18.Gür E, Binkhamis G, Kluk K. Effects of multiple sclerosis on the audio-vestibular system: a systematic review. BMJ Open 2022;12(8):e060540. doi: 10.1136/bmjopen-2021-060540.
- 19.Danesh-Sani SA, Rahimdoost A, Soltani M et al. Clinical assessment of orofacial manifestations in 500 patients with multiple sclerosis. J Oral Maxillofac Surg 2013;71(2):290-4. doi: 10.1016/j.joms.2012.05.008.
- 20.Chemaly D, Lefrançois A, Pérusse R. Oral and maxillofacial manifestations of multiple sclerosis. J Can Dent Assoc 2000;66(11):600-5.
- 21.Hooge JP, Redekop WK. Trigeminal neuralgia in multiple sclerosis. Neurol 1995;45:1294-6.
- 22.Fukazawa T, Moriwaka F, Hamada K et al. Facial palsy in multiple sclerosis. J Neurol 1997;244:631-3.
- 23.Calcagno P, Ruoppolo G, Grasso MG et al. Dysphagia in multiple sclerosis—Prevalence and prognostic factors. Acta Neurol Scand 2002;105:40-3. doi: 10.1034/j.1600-0404.2002.10062.x.
- 24.Kovac Z, Uhac I, Buković D et al. Oral health status and temporomandibular disorders in multiple sclerosis patients. Coll Antropol 2005;29(2):441-4.
- 25.Sexton C, Lalloo R, Stormon N et al. Oral health and behaviours of people living with Multiple Sclerosis in Australia. Community Dent Oral Epidemiol 2019;47:201-9.
- 26.https://www.webmd.com/multiple-sclerosis/ms-treatment
- 27.College of dental hygienists of Ontario. Multiple sclerosis. https://www.cda-adc.ca/jcda/vol-66/issue-11/600.pdf.
- 28.Cockburn N, Pateman K, Taing MW et al. Managing the oral side effects of medications used to treat multiple sclerosis. Aust Dent J 2017;62:331-6.
- 29.www.drugs.com
- 30.Multiple Sclerosis Society (MS Society UK). How can MS symptoms affect oral health? https://www.mssociety.org.uk/about-ms/signs-and-symptoms/oral-health.
- 31.https://penndentalmedicine.org/patient-information/dentist-for-special-needs/multiple-sclerosis-and-dentist/
- 32.Costa C, Santiago H, Pereira S et al. Oral Health Status and Multiple Sclerosis: Classic and Non-Classic Manifestations—Case Report. Diseases 2022;10:62. https:// doi.org/10.3390/diseases10030062./
- 33.National Multiple Sclerosis Society. Dental Health. https://www.nationalmssociety.org/nationalmssociety/media/msnationalfiles/brochures/brochure-dental-health.pdf/
- 34.WebMD. Drugs & Medications A–Z. Available at: webmd.com/drugs/indexdrugs. aspx.
- 35.Gallud L, Bagan JV, Cervelló A et al. Multiple sclerosis as first manifestation in oral and facial area: Presentation of four cases. Med Oral Patol Oral Cir Bucal 2006 ;11(2):E141-5.
- 36.Weyant RJ, Tracy SL, Anselmo TT et al; American Dental Association Council on Scientific Affairs Expert Panel on Topical Fluoride Caries Preventive Agents. Topical fluoride for caries prevention: executive summary of the updated clinical recommendations and supporting systematic review. J Am Dent Assoc 2013;144(11):1279-91. doi: 10.14219/jada.archive.2013.0057.
- 37.Hajeer S, Nasr F, Nabha S et al. Association between vitamin D deficiency and multiple sclerosis- MRI significance: A scoping review. Heliyon 2023;9(5):e15754. doi: 10.1016/j.heliyon.2023.e15754.
- 38.Complementary and Alternative Medicines and Multiple Sclerosis. https://www.nationalmssociety.org/Treating-MS/Complementary-Alternative-Medicines.