

Orthodontic Treatment and White Spot Lesions
Approximately 20 million comprehensive orthodontic cases were completed during a one-year survey period spanning 2005-2006.1American Dental Association. 2005-06 survey of services rendered. August 2017. Available at www.ada.org. Orthodontic treatment is most frequently performed in adolescents.1American Dental Association. 2005-06 survey of services rendered. August 2017. Available at www.ada.org. Options for orthodontic treatment include traditional removable appliances, fixed orthodontic appliances (FOA) and clear aligners. Comprehensive treatment is performed with FOA or clear aligners. In the United States, treatment is frequently performed using FOA. In addition, young adults have found treatment more acceptable since the introduction of clear aligners.2Jiang Q, Li J, Mei L, Du J, Levrini L, Abbate GM, Li H. Periodontal health during orthodontic treatment with clear aligners and fixed appliances: A meta-analysis. J Am Dent Assoc 2018;149(8):712-20.e12. Determining factors in treatment method include the complexity of treatment and patient preference.
Reported benefits of orthodontic care include improved esthetics, function and oral-health-related quality of life.3Benson PE, Vettore M, Javidi H. Does orthodontic treatment before the age of 18 years improve oral health-related quality of life? A systematic review and meta-analysis. Am J Orthod Dentofac Orthop 2017;151:644-55.,4Yun PW-L, Wong RW-K. Risks and complications in orthodontic treatment. Hong Kong Dent J 2006;3:5-22. Orthodontic treatment may also ultimately aid improved oral hygiene and benefit implant and restorative care-related esthetic outcomes.5Borzabadi-Farahani A. Orthodontic considerations in restorative management of hypodontia patients with endosseous implants. J Oral Implantol 2012;38(6):779-91. However, as with other treatment, oral health challenges and potential complications can occur. Orthodontic decalcifications (orthodontic white spot lesions; WSL) are one of the most common complications for individuals treated with FOA.
Prevalence and Etiology of Orthodontic WSL
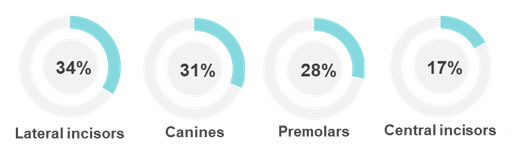
The reported prevalence of orthodontic WSL ranges from 0% to 97%.6Julien KC, Buschang PH, Campbell PM. Prevalence of white spot lesion formation during orthodontic treatment. Angle Orthod 2013;83(4):641-7. These lesions can occur within one month of placement of FOA.7O’Reilly MM, Featherstone JD. Demineralization and remineralization around orthodontic appliances: an in vivo study. Am J Orthod Dentofacial Orthop 1987;92(1):33-40.,8Gorelick L, Geiger AM, Gwinnett AJ. Incidence of white spot formation after bonding and banding. Am J Orthod 1982;81(2):93-8.,9Øgaard B, Rolla G, Arends J. Orthodontic appliances and enamel demineralization. Part 1. Lesion development. Am J Orthod Dentofacial Orthop 1988;94:68-73.,10Boersma JG, van der Veen MH, Lagerweij MD, Bokhout B, Prahl-Andersen B. Caries prevalence measured with QLF after treatment with fixed orthodontic appliances: influencing factors. Caries Res 2005;39(1):41-7. Most studies have used direct visualization and/or photography to identify orthodontic WSL. In one study using quantitative light fluorescence (QLF), which is more sensitive and objective than direct visualization and photography, 97% of subjects were found to experience orthodontic WSL, impacting on average 30% of buccal surfaces.10Boersma JG, van der Veen MH, Lagerweij MD, Bokhout B, Prahl-Andersen B. Caries prevalence measured with QLF after treatment with fixed orthodontic appliances: influencing factors. Caries Res 2005;39(1):41-7. In a second study, 95% of individuals had at least one lesion at the time of debonding.11Van der Veen, MH, Mattousch T, Boersma JG. Longitudinal development of caries lesions after orthodontic treatment evaluated by quantitative light-induced fluorescence. Am J Orthod Dentofacial Orthop 2007;131:223-8. The maxillary lateral incisors and canines are considered to be at greatest risk, followed by mandibular canines and bicuspids, and maxillary central incisors.6Julien KC, Buschang PH, Campbell PM. Prevalence of white spot lesion formation during orthodontic treatment. Angle Orthod 2013;83(4):641-7.,12Maxfield B, Hamdan A, Tufekci E, Shroff B, Best A, Lindauer SJ. Development of white spot lesions during orthodontic treatment: Perceptions of patients, parents, orthodontists, and general dentists. Am J Orthod Dentofac Orthop 2012;141:337-43. An incidence of 34%, 31%, 28% and 17% was found in one study for orthodontic WSL on maxillary lateral incisors, canines, premolars and central incisors, respectively.13Chapman JA, Roberts WE, Eckert GJ, Kula KS, González-Cabezas C. Risk factors for incidence and severity of white spot lesions during treatment with fixed orthodontic appliances. Am J Orthod Dentofacial Orthop 2010;138(2):188-94. (Figure 1)
By creating physical obstacles, the brackets and archwires of FOA reduce salivary clearance, complicate oral hygiene and result in increased plaque accumulation at adjacent sites.14Ireland AJ, Soro V, Sprague SV, Harradine NW, Day C, Al-Anezi S, Jenkinson HF, Sherriff M, Dymock D, Sandy JR. The effects of different orthodontic appliances upon microbial communities. Orthod Craniofac Res 2014;17(2):115-23. ,15Attin R, Thon C, Schlagenhauf U, Werner C, Wiegand A, Hannig C, Attin T. Recolonization of mutans streptococci on teeth with orthodontic appliances after antimicrobial therapy. Eur J Orthod 2005;27(5):489-93. WSL develop as a result of subsurface loss of minerals, caused by repeated demineralization by bacterial acids. The tooth structure thereby becomes less dense, altering the optical properties of the tooth structure with differences in light refraction. This results in a chalky, white appearance.
Rapid shifts in the intra-oral flora have been observed after patients receive FOA, and bacterial colonization on and adjacent to FOA by Streptococcus-mutans (S. mutans) and Lactobacilli occurs.14Ireland AJ, Soro V, Sprague SV, Harradine NW, Day C, Al-Anezi S, Jenkinson HF, Sherriff M, Dymock D, Sandy JR. The effects of different orthodontic appliances upon microbial communities. Orthod Craniofac Res 2014;17(2):115-23. ,16Forsberg CM, Brattstrom V, Malmberg E, Nord CE. Ligature wires and elastomeric rings: two methods of ligation, and their association with microbial colonization of Streptococcus mutans and lactobacilli. Eur J Orthod 1991;13(5):416-20.,17Hamdan AM, Maxfield BJ, Tüfekçi E, Shroff B, Lindauer SJ. Preventing and treating white-spot lesions associated with orthodontic treatment: a survey of general dentists and orthodontists. J Am Dent Assoc 2012;143(7):777-83. A diverse microflora has also been found in children receiving FOA. In one study, a positive association was found for Scardovia-wiggsiae and orthodontic WSL, and a negative association for Cardiobacterium-hominis.18Tanner AC, Sonis AL, Lif Holgerson P, Starr JR, Nunez Y, Kressirer CA, Paster BJ, Johansson I.. White-spot lesions and gingivitis microbiotas in orthodontic patients. J Dent Res 2012;91(9):853-8. Further, FOA component materials themselves influence the microbial shift.14Ireland AJ, Soro V, Sprague SV, Harradine NW, Day C, Al-Anezi S, Jenkinson HF, Sherriff M, Dymock D, Sandy JR. The effects of different orthodontic appliances upon microbial communities. Orthod Craniofac Res 2014;17(2):115-23. ,16Forsberg CM, Brattstrom V, Malmberg E, Nord CE. Ligature wires and elastomeric rings: two methods of ligation, and their association with microbial colonization of Streptococcus mutans and lactobacilli. Eur J Orthod 1991;13(5):416-20.
In one study, the relative risk for orthodontic WSL was 3.40, 3.12 and 2.83 for pre-existing WSL, poor oral hygiene during and prior to treatment, respectively.6Julien KC, Buschang PH, Campbell PM. Prevalence of white spot lesion formation during orthodontic treatment. Angle Orthod 2013;83(4):641-7. (Figure 2)
Risk factors include poor oral hygiene prior to orthodontic treatment and/or following treatment initiation, preadolescence at start of treatment, frequent intake of fermentable carbohydrates during treatment, not drinking milk at mealtimes, over-etching of the enamel surface prior to bonding, pre-existing WSL and past caries experience.6Julien KC, Buschang PH, Campbell PM. Prevalence of white spot lesion formation during orthodontic treatment. Angle Orthod 2013;83(4):641-7.,13Chapman JA, Roberts WE, Eckert GJ, Kula KS, González-Cabezas C. Risk factors for incidence and severity of white spot lesions during treatment with fixed orthodontic appliances. Am J Orthod Dentofacial Orthop 2010;138(2):188-94. ,18Tanner AC, Sonis AL, Lif Holgerson P, Starr JR, Nunez Y, Kressirer CA, Paster BJ, Johansson I.. White-spot lesions and gingivitis microbiotas in orthodontic patients. J Dent Res 2012;91(9):853-8.,19Knösel M, Bojes M, Jung K, Ziebolz D. Increased susceptibility for white spot lesions by surplus orthodontic etching exceeding bracket base area. Am J Orthod Dentofacial Orthop 2012;141:574-82.,20Shungin D, Olsson AI, Persson M. Orthodontic treatment-related white spot lesions: a 14-year prospective quantitative follow-up, including bonding material assessment. Am J Orthod Dentofacial Orthop 2010;138(2):136.e1-8. (Table 1)
| Table 1. Risk factors for orthodontic WSL |
|---|
| Poor oral hygiene prior to orthodontic treatment |
| Poor oral hygiene after placement of FOA |
| Preadolescence at start of treatment |
| Frequent intake of fermentable carbohydrates |
| Not drinking milk during mealtimes |
| Over-etching of the enamel surface prior to bonding |
| Pre-existing WSL and past caries experience |
Oral Hygiene
Thorough oral hygiene during orthodontic treatment is crucial. Plaque control can be achieved mechanically and with chemotherapeutics. Both manual and electric toothbrushes are effective when used properly. Manual brushes with soft bristles that are designed with a V-cut encourage contact of the brush with the tooth surface adjacent to brackets and are also available with firmer inner bristles and soft outer bristles that reach the gumline and outer areas of the tooth surface. In addition, multi-tufted manual brushes were found in one study to be more effective than electric brushes.21Trimpeneers LM, Wijgaerts IA, Grognard NA, Dermaut LR, Adriaens PA. Effect of electric toothbrushes versus manual toothbrushes on removal of plaque and periodontal status during orthodontic treatment. Am J Orthod Dentofacial Orthop 1997;111(5):492-7. Interactive electric/power toothbrushes are now available that coach patients on effective brushing. In one study, interactive brushing was found to result in greater plaque reduction and greater patient motivation compared to use of a manual brush.22Erbe C, Klees V, Braunbeck F, Ferrari-Peron P, Ccahuana-Vasquez RA, Timm H, Grender J, Cunningham P, Adam R, Wehrbein H. Comparative assessment of plaque removal and motivation between a manual toothbrush and an interactive power toothbrush in adolescents with fixed orthodontic appliances: A single-center, examiner-blind randomized controlled trial. Am J Orthod Dentofacial Orthop 2019;155(4):462-72. At a recent consensus conference, it was concluded that power brushes may increase the likelihood of compliance.23Bain C, Sayed AA, Kaklamanos EG, Kazi HA. Toothbrushing-should we advise mechanical or power brushes? Results of an international delphi conference. J Contemp Dent Pract 2018;19(10):1169-73.
Interdental cleaning is challenging, and more so for patients wearing FOA. Options include using floss with a floss threader, floss with a thickened end, manual interdental brushes and soft latex-free interdental cleaners. Mechanical interdental cleaning can be performed using a powered air flosser or an irrigating device/water flosser which patients may find easier to use than a manual device and which were found in separate studies to be effective in reducing gingivitis in orthodontic patients.24Nammi K, Starke EM, Ou SS, Ward M, Jenkins W, Milleman JL, Milleman KR. The effects of use of a powered and a manual home oral hygiene regimen on plaque and gum health in an orthodontic population. J Clin Dent 2019;30(Spec No A):A1-8.,25Sharma NC, Lyle DM, Qaqish JG, Galustians J, and Schuller R. Effect of a dental water jet with orthodontic tip on plaque and bleeding in adolescent patients with fixed orthodontic appliances. Am J Orthod Dentofac Orthop 2008;133(4):565-7. In addition, use of an antimicrobial rinse may help to reduce the intraoral microbial load. In selecting an antimicrobial mouth rinse, consideration must be given to potential side effects.
Preventive Care
Preventive care is essential to inhibit the development of orthodontic WSL and dental caries in general. Current recommendations for patients at risk for dental caries include periodic application of in-office topical fluoride (5% sodium fluoride varnish (or 1.23% APF gel for individuals age 6 and over)), fluoride dentifrice and other home use preventive products.26Weyant RJ, Tracy SL, Anselmo T, Beltrán-Aguilar ED, Donly KJ, Frese WA et al; American Dental Association Council on Scientific Affairs Expert Panel on Topical Fluoride Caries Preventive Agents. Topical fluoride for caries prevention. J Am Dent Assoc 2013;144(11):1279-91. More frequent applications of in-office fluorides are necessary for patients at higher risk of dental caries. In-office fluoride varnish can be applied specifically around the brackets, offers high fluoride release, and penetrates thin amounts of dental biofilm27Seppä L. Effect of dental plaque on fluoride uptake by enamel from a sodium fluoride varnish in vivo. Caries Res 1983;17(1):71-5.. Studies on the use of fluoride varnishes for the inhibition of orthodontic WSL are heterogeneous. However, in vitro and in vivo studies support the use of fluoride varnishes.28Ogaard B, Duschner H, Ruben J, Arends J. Microradiography and confocal laser scanning microscopy applied to enamel lesions formed in vivo with and without fluoride varnish treatment. Eur J Oral Sci 1996;104(4 Pt 1):378-83.,29Vivaldi-Rodrigues G, Demito CF, Bowman SJ, et al. The effectiveness of a fluoride varnish in preventing the development of white spot lesions. World J Orthod 2006;7:138-44.,30Alavi S, Yaraghi N. The effect of fluoride varnish and chlorhexidine gel on white spots and gingival and plaque indices in fixed orthodontic patients: A placebo-controlled study. Dent Res J (Isfahan) 2018;15(4):276-82. In another study, 5% sodium fluoride varnish reduced the WSL index, plaque and gingivitis compared to placebo or control in patients wearing FOA.30Alavi S, Yaraghi N. The effect of fluoride varnish and chlorhexidine gel on white spots and gingival and plaque indices in fixed orthodontic patients: A placebo-controlled study. Dent Res J (Isfahan) 2018;15(4):276-82. In addition, in a recent meta-analysis 5% sodium fluoride varnish was found to be most effective for arresting and reversing non-cavitated caries lesions on buccal surfaces.31Urquhart O, Tampi MP, Pilcher L, Slayton RL, Araujo MWB, Fontana M, Guzmán-Armstrong S, Nascimento MM, Nový BB, Tinanoff N, Weyant RJ, Wolff MS, Young DA, Zero DT, Brignardello-Petersen R, Banfield L, Parikh A, Joshi G, Carrasco-Labra A. Nonrestorative treatments for caries: Systematic review and network meta-analysis. J Dent Res 2019;98(1):14-26.
Fluoride dentifrices are recommended with brushing at least twice daily. Use of an antimicrobial toothpaste that contains fluoride also helps to reduce plaque and gingivitis, and to control dental caries. A dose-response exists for fluoride dentifrices and, for higher-risk patients, prescription-level fluoride pastes or gels (5,000 ppm) may be recommended. In a recent randomized controlled clinical trial with more than 400 adolescents, use of 5,000 ppm fluoride was found to reduce the formation of orthodontic WSL in maxillary bicuspids and anterior teeth by 32% compared to use of an over-the-counter dentifrice.32Sonesson M, Twetman S, Bondemark L. Effectiveness of high-fluoride toothpaste on enamel demineralization during orthodontic treatment-a multicenter randomized controlled trial. Eur J Orthod 2014;36(6):678-82.
Adjunctive daily use of a fluoride rinse elevates salivary and plaque fluoride levels. Rinses containing 0.05% sodium fluoride, or 0.044% acidulated phosphate fluoride, have been shown to significantly reduce WSL in orthodontic patients.33Geiger AM, Gorelick L, Gwinnett AJ, Benson BJ. Reducing white spot lesions in orthodontic populations with fluoride rinsing. Am J Orthod Dentofac Orthop 1992;101(5):403-7.,34Hirschfield HE. Control of decalcification by use of fluoride mouthrinse. ASDC J Dent Child 1978;45:458-60. The use of calcium-based technologies together with fluoride has also been recommended to increase the availability of calcium ions. In a recent systematic review, it was concluded that products containing fluoride and/or casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) are of benefit in reducing WSL.35Lopatiene K, Borisovaite M, Lapenaite E. Prevention and treatment of white spot lesions during and after treatment with fixed orthodontic appliances: A systematic literature review. J Oral Maxillofac Res 2016;7(2):e1. As an adjunct, use of xylitol may also be recommended for patients at risk for dental caries.36Rethman MP, Beltrán-Aguilar ED, Billings RJ, Burne RA, Clark M, Donly KJ, Hujoel PP, Katz BP, Milgrom P, Sohn W, Stamm JW, Watson G, Wolff M, Wright T, Zero D, Aravamudhan K, Frantsve-Hawley J, Meyer DM; for the American Dental Association Council on Scientific Affairs Expert Panel on Nonfluoride Caries-Preventive Agents. Nonfluoride caries-preventive agents. Executive summary of evidence-based clinical recommendations. J Am Dent Assoc 2011;142(9):1065-71. Since chewing gum is not generally recommended for patients wearing FOA, other options include xylitol-containing lozenges or candies. More research is required to clarify the most effective protocols for the prevention of WSL.
| Table 2. Preventive care products |
|---|
| 5% sodium fluoride varnish – frequency based on risk level |
| Fluoride toothpaste |
| 5,000 ppm fluoride paste or gel |
| Over-the-counter fluoride rinse |
| Calcium-based technologies – CPP-ACP |
| Antimicrobial products |
| Adjunctive use of xylitol |
Figure 3. Result of non-compliance
Risk Assessment and Patient Compliance
Patient compliance with treatment, oral hygiene and preventive measures is crucial for effective home care and desirable outcomes.37Hasegawa Jr TK, Matthews Jr M, Taylor R. Plaque, puberty, and noncompliance — the orthodontic dilemma. Tex Dent J 2002;119(7):645-7. In one study, less than 15% of patients followed home care instructions on rinsing.33Geiger AM, Gorelick L, Gwinnett AJ, Benson BJ. Reducing white spot lesions in orthodontic populations with fluoride rinsing. Am J Orthod Dentofac Orthop 1992;101(5):403-7. Sixty-nine percent of general dentists in one survey reported treating orthodontic WSL. Further, 37% of orthodontists reported removing FOA as a result of poor patient compliance with home care.18Tanner AC, Sonis AL, Lif Holgerson P, Starr JR, Nunez Y, Kressirer CA, Paster BJ, Johansson I.. White-spot lesions and gingivitis microbiotas in orthodontic patients. J Dent Res 2012;91(9):853-8. (Figure 3)
Prior to orthodontic treatment, a caries risk assessment should be performed, and a discussion held with patients and parents on the need for thorough home care. In patients with poor oral hygiene, improvement in oral hygiene should occur prior to beginning orthodontic treatment. Signed informed consent forms regarding treatment, risks and benefits are necessary, including the need for thorough home care and compliance. At the start of treatment, oral hygiene instruction showing patients how to best clean around brackets and under archwires is essential. Further, repeated education and patient motivation should be provided at each patient visit during treatment.
Managing post-treatment WSL
Some orthodontic WSL will regress/reverse with use of fluoride toothpaste alone after debonding. Using QLF, regression of WSL was found to occur mainly in the first 6 weeks after debonding and to some extent over a period of 6 months.11Van der Veen, MH, Mattousch T, Boersma JG. Longitudinal development of caries lesions after orthodontic treatment evaluated by quantitative light-induced fluorescence. Am J Orthod Dentofacial Orthop 2007;131:223-8. Complete reversal of WSL has been found with use of fluoride dentifrice plus 0.05% sodium fluoride rinse.11Van der Veen, MH, Mattousch T, Boersma JG. Longitudinal development of caries lesions after orthodontic treatment evaluated by quantitative light-induced fluorescence. Am J Orthod Dentofacial Orthop 2007;131:223-8. In systematic reviews, 5% sodium fluoride varnish was found to help remineralize WSL.38Fernández-Ferrer L, Vicente-Ruíz M, García-Sanz V, Montiel-Company JM, Paredes-Gallardo V, Almerich-Silla JM, Bellot-Arcís C. Enamel remineralization therapies for treating postorthodontic white-spot lesions: A systematic review. J Am Dent Assoc 2018;149(9):778-86.e2. ,39Höchli D, Hersberger-Zurfluh M, Papageorgiou SN, Eliades T. Interventions for orthodontically induced white spot lesions: a systematic review and meta-analysis. Eur J Orthod 2017;39(2):122-33. In addition, CPP-ACP paste has been found to help improve esthetics and reverse orthodontic WSL.35Lopatiene K, Borisovaite M, Lapenaite E. Prevention and treatment of white spot lesions during and after treatment with fixed orthodontic appliances: A systematic literature review. J Oral Maxillofac Res 2016;7(2):e1.
For recalcitrant WSL that do not regress or resolve with remineralization therapy, minimally invasive treatment options include tooth whitening, microabrasion, and resin infiltration. Tooth whitening lightens the tooth structure surrounding WSL, thereby reducing differences in color and masking these lesions. Microabrasion may be performed using a commercially-available microabrasion paste (or pumice slurry), or in combination with etching of the site(s).40Croll T, Donly K. Enamel microabrasion for removal of decalcification, dysmineralization, and surface defects. Am J Esthet Dent 2013;3:92-9. Microabrasion can significantly improve esthetics. In addition, both microabrasion and tooth whitening can be performed. A third technique involves etching and infiltration of the WSL with a low-viscosity resin. This method fills the defect, thereby altering its optical properties and masking it.41Knösel M, Eckstein A, Helms HJ. Long-term follow-up of camouflage effects following resin infiltration of post orthodontic white-spot lesions in vivo. Angle Orthod 2019;89(1):33-39. Resin infiltration has also been shown to arrest WSL.42Cazzolla AP, De Franco AR, Lacaita M, Lacarbonara V. Efficacy of 4-year treatment of icon infiltration resin on postorthodontic white spot lesions. Case Reports 2018;2018:bcr-2018-225639.
Conclusions
A risk assessment and patient education should occur prior to placement of FOA as well as needed improvements in oral hygiene. Patients and parents must be cognizant of the need for home care and preventive care during treatment and must also commit to this. Effective oral hygiene and preventive care is essential to optimize treatment outcomes.
References
- 1.American Dental Association. 2005-06 survey of services rendered. August 2017. Available at www.ada.org.
- 2.Jiang Q, Li J, Mei L, Du J, Levrini L, Abbate GM, Li H. Periodontal health during orthodontic treatment with clear aligners and fixed appliances: A meta-analysis. J Am Dent Assoc 2018;149(8):712-20.e12.
- 3.Benson PE, Vettore M, Javidi H. Does orthodontic treatment before the age of 18 years improve oral health-related quality of life? A systematic review and meta-analysis. Am J Orthod Dentofac Orthop 2017;151:644-55.
- 4.Yun PW-L, Wong RW-K. Risks and complications in orthodontic treatment. Hong Kong Dent J 2006;3:5-22.
- 5.Borzabadi-Farahani A. Orthodontic considerations in restorative management of hypodontia patients with endosseous implants. J Oral Implantol 2012;38(6):779-91.
- 6.Julien KC, Buschang PH, Campbell PM. Prevalence of white spot lesion formation during orthodontic treatment. Angle Orthod 2013;83(4):641-7.
- 7.O’Reilly MM, Featherstone JD. Demineralization and remineralization around orthodontic appliances: an in vivo study. Am J Orthod Dentofacial Orthop 1987;92(1):33-40.
- 8.Gorelick L, Geiger AM, Gwinnett AJ. Incidence of white spot formation after bonding and banding. Am J Orthod 1982;81(2):93-8.
- 9.Øgaard B, Rolla G, Arends J. Orthodontic appliances and enamel demineralization. Part 1. Lesion development. Am J Orthod Dentofacial Orthop 1988;94:68-73.
- 10.Boersma JG, van der Veen MH, Lagerweij MD, Bokhout B, Prahl-Andersen B. Caries prevalence measured with QLF after treatment with fixed orthodontic appliances: influencing factors. Caries Res 2005;39(1):41-7.
- 11.Van der Veen, MH, Mattousch T, Boersma JG. Longitudinal development of caries lesions after orthodontic treatment evaluated by quantitative light-induced fluorescence. Am J Orthod Dentofacial Orthop 2007;131:223-8.
- 12.Maxfield B, Hamdan A, Tufekci E, Shroff B, Best A, Lindauer SJ. Development of white spot lesions during orthodontic treatment: Perceptions of patients, parents, orthodontists, and general dentists. Am J Orthod Dentofac Orthop 2012;141:337-43.
- 13.Chapman JA, Roberts WE, Eckert GJ, Kula KS, González-Cabezas C. Risk factors for incidence and severity of white spot lesions during treatment with fixed orthodontic appliances. Am J Orthod Dentofacial Orthop 2010;138(2):188-94.
- 14.Ireland AJ, Soro V, Sprague SV, Harradine NW, Day C, Al-Anezi S, Jenkinson HF, Sherriff M, Dymock D, Sandy JR. The effects of different orthodontic appliances upon microbial communities. Orthod Craniofac Res 2014;17(2):115-23.
- 15.Attin R, Thon C, Schlagenhauf U, Werner C, Wiegand A, Hannig C, Attin T. Recolonization of mutans streptococci on teeth with orthodontic appliances after antimicrobial therapy. Eur J Orthod 2005;27(5):489-93.
- 16.Forsberg CM, Brattstrom V, Malmberg E, Nord CE. Ligature wires and elastomeric rings: two methods of ligation, and their association with microbial colonization of Streptococcus mutans and lactobacilli. Eur J Orthod 1991;13(5):416-20.
- 17.Hamdan AM, Maxfield BJ, Tüfekçi E, Shroff B, Lindauer SJ. Preventing and treating white-spot lesions associated with orthodontic treatment: a survey of general dentists and orthodontists. J Am Dent Assoc 2012;143(7):777-83.
- 18.Tanner AC, Sonis AL, Lif Holgerson P, Starr JR, Nunez Y, Kressirer CA, Paster BJ, Johansson I.. White-spot lesions and gingivitis microbiotas in orthodontic patients. J Dent Res 2012;91(9):853-8.
- 19.Knösel M, Bojes M, Jung K, Ziebolz D. Increased susceptibility for white spot lesions by surplus orthodontic etching exceeding bracket base area. Am J Orthod Dentofacial Orthop 2012;141:574-82.
- 20.Shungin D, Olsson AI, Persson M. Orthodontic treatment-related white spot lesions: a 14-year prospective quantitative follow-up, including bonding material assessment. Am J Orthod Dentofacial Orthop 2010;138(2):136.e1-8.
- 21.Trimpeneers LM, Wijgaerts IA, Grognard NA, Dermaut LR, Adriaens PA. Effect of electric toothbrushes versus manual toothbrushes on removal of plaque and periodontal status during orthodontic treatment. Am J Orthod Dentofacial Orthop 1997;111(5):492-7.
- 22.Erbe C, Klees V, Braunbeck F, Ferrari-Peron P, Ccahuana-Vasquez RA, Timm H, Grender J, Cunningham P, Adam R, Wehrbein H. Comparative assessment of plaque removal and motivation between a manual toothbrush and an interactive power toothbrush in adolescents with fixed orthodontic appliances: A single-center, examiner-blind randomized controlled trial. Am J Orthod Dentofacial Orthop 2019;155(4):462-72.
- 23.Bain C, Sayed AA, Kaklamanos EG, Kazi HA. Toothbrushing-should we advise mechanical or power brushes? Results of an international delphi conference. J Contemp Dent Pract 2018;19(10):1169-73.
- 24.Nammi K, Starke EM, Ou SS, Ward M, Jenkins W, Milleman JL, Milleman KR. The effects of use of a powered and a manual home oral hygiene regimen on plaque and gum health in an orthodontic population. J Clin Dent 2019;30(Spec No A):A1-8.
- 25.Sharma NC, Lyle DM, Qaqish JG, Galustians J, and Schuller R. Effect of a dental water jet with orthodontic tip on plaque and bleeding in adolescent patients with fixed orthodontic appliances. Am J Orthod Dentofac Orthop 2008;133(4):565-7.
- 26.Weyant RJ, Tracy SL, Anselmo T, Beltrán-Aguilar ED, Donly KJ, Frese WA et al; American Dental Association Council on Scientific Affairs Expert Panel on Topical Fluoride Caries Preventive Agents. Topical fluoride for caries prevention. J Am Dent Assoc 2013;144(11):1279-91.
- 27.Seppä L. Effect of dental plaque on fluoride uptake by enamel from a sodium fluoride varnish in vivo. Caries Res 1983;17(1):71-5.
- 28.Ogaard B, Duschner H, Ruben J, Arends J. Microradiography and confocal laser scanning microscopy applied to enamel lesions formed in vivo with and without fluoride varnish treatment. Eur J Oral Sci 1996;104(4 Pt 1):378-83.
- 29.Vivaldi-Rodrigues G, Demito CF, Bowman SJ, et al. The effectiveness of a fluoride varnish in preventing the development of white spot lesions. World J Orthod 2006;7:138-44.
- 30.Alavi S, Yaraghi N. The effect of fluoride varnish and chlorhexidine gel on white spots and gingival and plaque indices in fixed orthodontic patients: A placebo-controlled study. Dent Res J (Isfahan) 2018;15(4):276-82.
- 31.Urquhart O, Tampi MP, Pilcher L, Slayton RL, Araujo MWB, Fontana M, Guzmán-Armstrong S, Nascimento MM, Nový BB, Tinanoff N, Weyant RJ, Wolff MS, Young DA, Zero DT, Brignardello-Petersen R, Banfield L, Parikh A, Joshi G, Carrasco-Labra A. Nonrestorative treatments for caries: Systematic review and network meta-analysis. J Dent Res 2019;98(1):14-26.
- 32.Sonesson M, Twetman S, Bondemark L. Effectiveness of high-fluoride toothpaste on enamel demineralization during orthodontic treatment-a multicenter randomized controlled trial. Eur J Orthod 2014;36(6):678-82.
- 33.Geiger AM, Gorelick L, Gwinnett AJ, Benson BJ. Reducing white spot lesions in orthodontic populations with fluoride rinsing. Am J Orthod Dentofac Orthop 1992;101(5):403-7.
- 34.Hirschfield HE. Control of decalcification by use of fluoride mouthrinse. ASDC J Dent Child 1978;45:458-60.
- 35.Lopatiene K, Borisovaite M, Lapenaite E. Prevention and treatment of white spot lesions during and after treatment with fixed orthodontic appliances: A systematic literature review. J Oral Maxillofac Res 2016;7(2):e1.
- 36.Rethman MP, Beltrán-Aguilar ED, Billings RJ, Burne RA, Clark M, Donly KJ, Hujoel PP, Katz BP, Milgrom P, Sohn W, Stamm JW, Watson G, Wolff M, Wright T, Zero D, Aravamudhan K, Frantsve-Hawley J, Meyer DM; for the American Dental Association Council on Scientific Affairs Expert Panel on Nonfluoride Caries-Preventive Agents. Nonfluoride caries-preventive agents. Executive summary of evidence-based clinical recommendations. J Am Dent Assoc 2011;142(9):1065-71.
- 37.Hasegawa Jr TK, Matthews Jr M, Taylor R. Plaque, puberty, and noncompliance — the orthodontic dilemma. Tex Dent J 2002;119(7):645-7.
- 38.Fernández-Ferrer L, Vicente-Ruíz M, García-Sanz V, Montiel-Company JM, Paredes-Gallardo V, Almerich-Silla JM, Bellot-Arcís C. Enamel remineralization therapies for treating postorthodontic white-spot lesions: A systematic review. J Am Dent Assoc 2018;149(9):778-86.e2.
- 39.Höchli D, Hersberger-Zurfluh M, Papageorgiou SN, Eliades T. Interventions for orthodontically induced white spot lesions: a systematic review and meta-analysis. Eur J Orthod 2017;39(2):122-33.
- 40.Croll T, Donly K. Enamel microabrasion for removal of decalcification, dysmineralization, and surface defects. Am J Esthet Dent 2013;3:92-9.
- 41.Knösel M, Eckstein A, Helms HJ. Long-term follow-up of camouflage effects following resin infiltration of post orthodontic white-spot lesions in vivo. Angle Orthod 2019;89(1):33-39.
- 42.Cazzolla AP, De Franco AR, Lacaita M, Lacarbonara V. Efficacy of 4-year treatment of icon infiltration resin on postorthodontic white spot lesions. Case Reports 2018;2018:bcr-2018-225639.