

Periodontal Risk Assessment
Periodontal disease (PD) is multifactorial and the leading cause of tooth loss.1Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJ, Marcenes W. Global burden of severe periodontitis in 1990–2010: A systematic review and meta-regression. J Dent Res 2014;93:1045-53. Globally, approximately 50% of adults experience PD, with an estimated prevalence of 10.7% for severe periodontitis.1Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJ, Marcenes W. Global burden of severe periodontitis in 1990–2010: A systematic review and meta-regression. J Dent Res 2014;93:1045-53.,2Nazir MA. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int J Health Sci 2017;11:72–80. (Figure 1) In the United States, an estimated 8.7%, 30% and 8.5% of adults 30 years-of-age and over have mild, moderate and severe periodontitis, respectively.3Eke PI, Dye BA, Wei L, Thornton-Evans GO, Genco RJ, et al. Prevalence of periodontitis in adults in the United States: 2009 and 2010. J Dent Res 2012;91(10):914-20. By age 65, an estimated 57% of adults in the United States have mild or moderate periodontitis and 11% have severe periodontitis.4Eke PI, Wei L, Borgnakke WS, Zhang X, Lu H, McGuire LC, Genco RJ. Periodontitis prevalence in adults ≥ 65 years of age, in the USA. Periodontol 2000 2016;72(1):76-95.
Figure 1. Global prevalence of PD
Biofilm-induced periodontal disease requires the presence of a subgingival microbiota. However, its onset and progression depend on the host response and modifying factors.5Lang NP, Bartold MP. Periodontal health. J Clin Periodontol 2018;45(Suppl 20):S9-16.,6Bartold PM. Lifestyle and periodontitis: The emergence of personalized periodontics. Periodontol 2000 2018 Oct;78(1):7-11.
In March 2018, a revised classification system for periodontal and peri-implant diseases and conditions was published and forms a basis for individualized care.7Caton JG, Armitage G, Berglundh T, Chapple ILC, Jepsen S, Kornman KS, Mealey BL, Papapanou PN, Sanz M, Tonetti MS. A new classification scheme for periodontal and peri-implant diseases and conditions – Introduction and key changes from the 1999 classification. J Periodontol 2018;89(Suppl 1):S1-8. Staging, extent and distribution of disease, and grading criteria based upon anticipated disease progression and response to therapy, are included in this classification. Further, smoking and diabetes mellitus are included as modifying risk factors for disease progression and response to therapy. In order to provide individualized care, a periodontal risk assessment is necessary to determine a patient’s risk for disease as well as the likelihood of disease progression and the potential response to treatment.8American Academy of Periodontology. Statement on risk assessment. J Periodontol 2008;79:202. Risk is dynamic and its assessment must be repeated periodically to determine changes in risk factors and risk level. Risk assessment can also improve decision-making.8American Academy of Periodontology. Statement on risk assessment. J Periodontol 2008;79:202.
Periodontal risk assessment considers the multifactorial nature of PD and determines patients’ risk levels based on all of their existing risk factors.
Periodontal Risk Factors
Risk factors are defined as “any attribute, characteristic or exposure of an individual that increases the likelihood of developing a disease or injury.”9World Health Organization. Risk factors. Available at: https://www.who.int/topics/risk_factors/en/. Environmental risk factors for the onset, progression and severity of periodontal disease include tobacco use, alcohol consumption, poor nutrition, stress, some medications, and substance abuse.5Lang NP, Bartold MP. Periodontal health. J Clin Periodontol 2018;45(Suppl 20):S9-16.,6Bartold PM. Lifestyle and periodontitis: The emergence of personalized periodontics. Periodontol 2000 2018 Oct;78(1):7-11.,10Chapple IL, Genco R, Working Group 2 of the Joint EFP/AAP Workshop. Diabetes and periodontal diseases. Consensus report of the Joint EFP/AAP Workshop on periodontitis and systemic diseases. J Periodontol 2013;84(4):S106-12.,11Albandar JM, Streckfus CF, Adesanya MR, Winn DM. Cigar, pipe, and cigarette smoking as risk factors for periodontal disease and tooth loss. J Periodontol 2000;71(12):1874-81.,12Shariff JA, Ahluwalia KP, Papapanou PN. Relationship between frequent recreational cannabis (marijuana and hashish) use and periodontitis in adults in the United States: Nhanes 2011-12. J Periodontol 2017;88(3):273-80.,13Hach M, Holm-Pedersen P, Adegboye A, Avlund K. The effect of alcohol consumption on periodontitis in older Danes. Int J Dent Hyg 2015;12:1-7. Systemic risk factors for the onset and progression of PD include diabetes mellitus (poorly-controlled), pre-diabetes, obesity and weight gain.5Lang NP, Bartold MP. Periodontal health. J Clin Periodontol 2018;45(Suppl 20):S9-16.,14Suvan JE, Finer N, D’Aiuto F. Periodontal complications with obesity. Periodontol 2000 2018;78(1):98-128.,15American Dental Association. Electronic oral health risk assessment tools. SCDI White Paper No. 1074, 2013. Available at: http://www.ada.org/~/media/ADA/Science%20and%20Research/Files/ADAWhitePaperNo1074.pdf?la=en. Recent findings also suggest rheumatoid arthritis as a risk factor.16Scher JU, Ubeda C, Equinda M, Khanin R, Buischi Y, Viale A, Lipuma L, Attur M, Pillinger MH, Weissmann G, Littman DR, Pamer EG, Bretz WA, Abramson SB. Periodontal disease and the oral microbiota in new onset rheumatoid arthritis. Arthritis Rheum 2012;64:3083-94.,17Berthelot J-M, Le Goff B. Rheumatoid arthritis and periodontal disease. Joint Bone Spine 2010;77(6):537-41. Local risk factors include poor oral hygiene, bleeding on probing (BOP), pocket probing depths (PPD), attachment loss (AL), furcation involvement, subgingival calculus and iatrogenic factors (e.g., restorations with defective subgingival margins).6Bartold PM. Lifestyle and periodontitis: The emergence of personalized periodontics. Periodontol 2000 2018 Oct;78(1):7-11.,16Scher JU, Ubeda C, Equinda M, Khanin R, Buischi Y, Viale A, Lipuma L, Attur M, Pillinger MH, Weissmann G, Littman DR, Pamer EG, Bretz WA, Abramson SB. Periodontal disease and the oral microbiota in new onset rheumatoid arthritis. Arthritis Rheum 2012;64:3083-94. Genetic polymorphism and epigenetics (whereby gene expression is altered through chemical changes to DNA and proteins) are also considered risk factors.6Bartold PM. Lifestyle and periodontitis: The emergence of personalized periodontics. Periodontol 2000 2018 Oct;78(1):7-11.,18Kurushima Y, Tsai PC, Castillo-Fernandez J, Couto Alves A, El-Sayed Moustafa JS, Le Roy C, Spector TD, Ide M, Hughes FJ, Small KS, Steves CJ, Bell JT. Epigenetic findings in periodontitis in UK twins: a cross-sectional study. Clin Epigenetics 2019;11(1):27. (Table 1)
| Table 1. Risk factors for periodontal disease | |
|---|---|
| Environmental risk factors | Tobacco use, alcohol consumption, nutrition, stress, some medications, substance abuse |
| Systemic risk factors | Diabetes mellitus, pre-diabetes, obesity, weight gain, genetics, epigenetics |
| Local risk factors | Poor oral hygiene, BOP, PPD, AL, furcation involvement, subgingival calculus, iatrogenic factors |
Periodontal Risk Assessment
Periodontal risk assessment requires a full periodontal examination, including radiographs, and a review of the patient’s medical and dental history. Risk assessment can be performed using forms developed in the dental office or available online. During the last two decades, several electronic risk assessment tools have been developed. Non-invasive diagnostic tests using salivary biomarkers are being used and continue to be researched.
Electronic Risk Assessment Tools
A number of criteria have been noted for electronic risk assessment tools.15American Dental Association. Electronic oral health risk assessment tools. SCDI White Paper No. 1074, 2013. Available at: http://www.ada.org/~/media/ADA/Science%20and%20Research/Files/ADAWhitePaperNo1074.pdf?la=en. These include privacy and security (at a minimum compliant with regulations), output that is easily understood by patients and dental professionals, output values that can adjusted reflecting changes in oral health status, ease of use, efficiency, precision and proven accuracy. In addition, they should aid clinical decision making, encourage treatment acceptance, embody evidence-based dentistry and best practices, and be clinically validated.15American Dental Association. Electronic oral health risk assessment tools. SCDI White Paper No. 1074, 2013. Available at: http://www.ada.org/~/media/ADA/Science%20and%20Research/Files/ADAWhitePaperNo1074.pdf?la=en.
Periodontal Risk Assessment Tools
The Periodontal Risk Calculator (PRC) was developed using 11 data points to assess risk for PD on a scale of 1 to 5 (lowest to highest level of risk).19Page RC, Krall EA, Martin J, Mancl L, Garcia RI. Validity and accuracy of a risk calculator in predicting periodontal disease. J Am Dent Assoc 2002;133(5):569-76. Smoking history, age, DM status, periodontal therapy received, PPD, BOP, subgingival restorations and calculus, vertical bone lesions, radiographic bone height and furcation involvement were included as risk factors.19Page RC, Krall EA, Martin J, Mancl L, Garcia RI. Validity and accuracy of a risk calculator in predicting periodontal disease. J Am Dent Assoc 2002;133(5):569-76.,20Page RC, Martin J, Krall EA, Mancl L, Garcia R. Longitudinal validation of a risk calculator for periodontal disease. J Clin Periodontol 2003;30:819-27. In a longitudinal study, a strong correlation was found for baseline risk scores, severity of PD and tooth loss.19Page RC, Krall EA, Martin J, Mancl L, Garcia RI. Validity and accuracy of a risk calculator in predicting periodontal disease. J Am Dent Assoc 2002;133(5):569-76. Subsequently, the Health Improvement in Dental Practice Model (HIDEP) with 17 data points was introduced in 2007.21Sandberg HCH, Fors UGH. The HIDEP model--a straightforward dental health care model for prevention-based practice management. Swed Dent J 2007;31(4):171-9.
The Oral Health Information Suite (OHIS; PreViser) provides validated risk assessment scores for PD, dental caries and oral cancer using the same scale as PRC and utilizing green amber red visuals in reports to signal low to high risk levels.22Page RC, Martin JA, Loeb CF. The Oral Health Information Suite (OHIS): Its use in the management of periodontal disease. J Dent Ed 2005;69(5):509-20. A similar ‘traffic-light’ methodology was proposed for data used in research on healthcare utilization for patients with cardiovascular disease.23Carrington MJ, Kok S, Jansen K, Stewart S. The Green, Amber, Red Delineation of Risk and Need (GARDIAN) management system: a pragmatic approach to optimizing heart health from primary prevention to chronic disease management. Eur J Cardiovasc Nurs 2013;12(4):337-45. The OHIS periodontal risk assessment utilizes 23 data points derived from the patient’s periodontal examination, medical and dental history, and disease scores on a scale of 1 (health) to 100 (severe periodontitis in all sextants) are included.22Page RC, Martin JA, Loeb CF. The Oral Health Information Suite (OHIS): Its use in the management of periodontal disease. J Dent Ed 2005;69(5):509-20.,24Martin JA, Page RC, Kaye EK, Hamed MT, Loeb CF. Periodontitis severity plus risk as a tooth loss predictor. J Periodontol 2009;80(2):202-9. The combination of risk and severity scores has been found to better predict tooth loss than disease risk alone.24Martin JA, Page RC, Kaye EK, Hamed MT, Loeb CF. Periodontitis severity plus risk as a tooth loss predictor. J Periodontol 2009;80(2):202-9. Individualized patient reports and suggested treatments are generated, and outcomes can be assessed.
In the United Kingdom, a dental insurance company developed an online tool (DEPPA) that used OHIS to assess risk for PD and its severity, dental caries and oral cancer. DEPPA included an Oral Health Status (OHS) score, utilizing information from clinicians and patients (satisfaction and perception on function, comfort, aesthetics).25Busby M, Chapple E, Matthews R, Chapple ILC. Practitioner evaluation of a novel online integrated oral health and risk assessment tool: a practice pilot. Br Dent J 2013;215(3):115-20.,26Delargy S, Busby M, McHugh S, Matthews R, Burke FJ. The reproducibility of the Denplan Oral Health Score (OHS) in general dental practitioners. Community Dent Health 2007;24:105-10. Another system uses a voice-activated application that automates charting, records periodontal data over periods of time, includes risk assessment, and delivers charts and a summary with patient recommendations.27Thyvalikakath T, Song M, Schleyer T. Perceptions and attitudes toward performing risk assessment for periodontal disease: a focus group exploration. BMC Oral Health 2018;18(1):90.
Risk assessment tools intended solely for use after initial periodontal therapy have also been developed.28Lang NP, Tonetti MS. Periodontal risk assessment (PRA) for patients in supportive periodontal therapy (SPT). Oral Health Prev Dent 2003;1:7-16. The Periodontal Risk Assessment tool (PRA) included 6 variables and was validated in a long-term study in patients with varying levels of risk and attending for periodontal maintenance.29Matuliene G, Studer R, Lang NP, Schmidlin K, Pjetursson BE, Salvi GE, Brägger U, Zwahlen M. Significance of Periodontal Risk Assessment on the recurrence of periodontitis and tooth loss. J Clin Periodontol 2010;37:191-9. Several retrospective studies have been conducted on PRA and modified PRAs.29Matuliene G, Studer R, Lang NP, Schmidlin K, Pjetursson BE, Salvi GE, Brägger U, Zwahlen M. Significance of Periodontal Risk Assessment on the recurrence of periodontitis and tooth loss. J Clin Periodontol 2010;37:191-9.,30Jansson H, Norderyd O. Evaluation of a periodontal risk assessment model in subjects with severe periodontitis. A 5-year retrospective study. Swed Dent J 2008;32(1):1-7.,31Chandra RV. Evaluation of a novel periodontal risk assessment model in patients presenting for dental care. Oral Health Prev Dent 2007;5(1):39-48.,32Leininger M, Tenenbaum H, Davideau J-L. Modified periodontal risk assessment score: long-term predictive value of treatment outcomes. A retrospective study. J Clin Periodontol 2010;37(5):427-35. The UniFe tool includes just 5 risk factors (smoking status, DM status, PPD, BOP, bone loss and age). While simpler than other methods, it was concluded in one study that further studies were required for validation.33Trombelli L, Farina R, Ferrari S, Pasetti P, Calura G. Comparison between two methods for periodontal risk assessment. Minerva Stomatol 2009;58:277-87.
Comparison of electronic and traditional periodontal risk assessment
Studies indicate greater accuracy using validated electronic methods compared to subjective methods. In one study, periodontists subjectively underestimated PD risk in the high-risk group with only 20% concurrence with objective risk assessment scores, and overestimated risk for low-risk patients.34Persson GR, Mancl LA, Martin JA, Page RC. Assessing periodontal disease risk. J Am Dent Assoc 2003;134(5):575-82. Among general dentists, variability was greater at all levels of risk.34Persson GR, Mancl LA, Martin JA, Page RC. Assessing periodontal disease risk. J Am Dent Assoc 2003;134(5):575-82. In a study using case presentations, while 88% of general dentists provided the same diagnosis for severe PD only 55% diagnosed gingivitis.35Martin JA, Grill AC, Matthews AG, Vena D, Thompson VP, Craig RG, Curro FA. Periodontal diagnosis affected by variation in terminology. Periodontol 2013;84:606-13. A need for standardized terminology was reported. In a systematic review of studies on five periodontal risk assessment tools, these were found to reliably identify patients’ risk for PD progression, and to predict progression and tooth loss in patients treated for PD.36Lang NP, Suvan JE, Tonetti MS. Risk factor assessment tools for the prevention of periodontitis progression a systematic review. J Clin Periodontol 2015;42(S16):S59-70. Electronic periodontal risk assessments can be automatically stored, and results compared over time.
Experiences and barriers for periodontal risk assessment tools
In a large group practice setting, dentists, dental hygienists and dental assistants were surveyed. After using a proprietary electronic clinical decision support program that included a periodontal risk assessment tool for 15 months, they reported greater belief that the process worked well and in the scientific validity of support tools.37Mertz E, Wides C, White J. Clinician attitudes, skills, motivations and experience following the implementation of clinical decision support tools in a large dental practice. J Evid Based Dent Pract 2017;17(1):1-12. Respondents were motivated by their perception that patient care, oral health and the patient experience had improved, while also reporting that stress and workload had increased.
OHIS was incorporated into an insurer’s pilot oral health and wellness dental benefit plan in the United States.38Martin J, Mills S, Foley ME. Innovative models of dental care delivery and coverage. Patient-centric dental benefits based on digital oral health risk assessment. Dent Clin N Am 2018;62:319-25. This enabled automated predetermination of evidence-based prevention and care for PD and dental caries, based on an individual’s risk level (moderate or high), and provided recommendations. Patients could participate if they signed up for an online assessment to obtain an oral health and wellness score, to help encourage them to manage their oral health.39Mills SE. Creating a risk-based model for dental benefit design. J Dent Hyg 2015;89(Suppl 1):24-6. Almost all insured employer groups signed up and 86% of providers in the region submitting claims to the insurer. Outcomes research is ongoing. High levels of satisfaction with the pilot program were reported in a survey of dentists. In addition, administrative costs were reduced through automation.
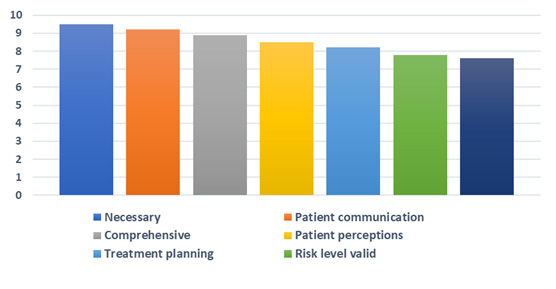
Figure 2. Scores for attributes of the pilot version of DEPPA
In the United Kingdom, 25 general dentists reported on their experiences using a pilot version of DEPPA.25Busby M, Chapple E, Matthews R, Chapple ILC. Practitioner evaluation of a novel online integrated oral health and risk assessment tool: a practice pilot. Br Dent J 2013;215(3):115-20. Seven of 10 questions assessed overall validity, effect on patient communication and treatment planning, patient perceptions, and its necessity, comprehensiveness and ease of use. The overall score of 8.5 out of 10 indicated a high degree of satisfaction. (Figure 2) Additionally, DEPPA was used to derive a capitated fee scale more heavily weighted by periodontal disease severity than prior fees, resulting in a satisfaction score of 8.25Busby M, Chapple E, Matthews R, Chapple ILC. Practitioner evaluation of a novel online integrated oral health and risk assessment tool: a practice pilot. Br Dent J 2013;215(3):115-20.
In contrast, in a recent focus group series with 27 dentists and 25 dental hygienists in dental practice, the majority reported performing subjective mental periodontal risk assessments.27Thyvalikakath T, Song M, Schleyer T. Perceptions and attitudes toward performing risk assessment for periodontal disease: a focus group exploration. BMC Oral Health 2018;18(1):90. Barriers cited for use of periodontal risk assessment tools included lack of/limited validation, insufficient validation in standard clinical settings, the need to emphasize whether/how these tools would be effective in helping to reduce a patient’s risk, the extra time required, reimbursement constraints for risk assessment and preventive care, and the difficulty of changing behaviors. Almost a third of participants reported using only paper charts.27Thyvalikakath T, Song M, Schleyer T. Perceptions and attitudes toward performing risk assessment for periodontal disease: a focus group exploration. BMC Oral Health 2018;18(1):90. (Table 2)
| Table 2. Barriers cited for use of periodontal risk assessment tools27Thyvalikakath T, Song M, Schleyer T. Perceptions and attitudes toward performing risk assessment for periodontal disease: a focus group exploration. BMC Oral Health 2018;18(1):90. |
|---|
| Lack of/limited validation |
| Insufficient validation in standard clinical settings |
| Need to emphasize whether/how they would effectively reduce a patient’s risk |
| Time/workload and reimbursement constraints |
| Difficulty of changing behavior |
Salivary Biomarkers
Non-invasive salivary tests are available for periodontal risk assessment, and a wide range of research is being conducted.6Bartold PM. Lifestyle and periodontitis: The emergence of personalized periodontics. Periodontol 2000 2018 Oct;78(1):7-11. Chairside salivary occult blood screening tests have been developed that use a paper strip impregnated with an anti-human hemoglobin monoclonal antibody.40Shimazaki Y, Akifusa S, Takeshita T, Shibata Y, Doi Y, Hata J, Ninomiya T, Hirakawa Y, Kiyohara Y, Yamashita Y. Effectiveness of the salivary occult blood test as a screening method for periodontal status J Periodontol. 2011;82(4):581-7. More research on the reliability and accuracy of this test has been recommended.41Reed SG, Manz M, Snipe SM, Ohshimna M, Wagner CL. Feasibility study of a salivary occult blood test to correlate with periodontal measures as indicators of periodontal inflammation in a population of pregnant women. J Oral Sci 2015;57(1): 55-8. Another salivary test, based on DNA-polymerase chain reaction, identifies periodontal pathogens and concentration, while unable to predict disease onset.42Kim JJ, Kim CJ, Camargo PM. Salivary biomarkers in the diagnosis of periodontal diseases. J Calif Dent Assoc. 2013;41(2):119-24. Host-related chemical mediators show potential as biomarkers.43Korte DL, Kinney J. Personalized medicine: an update of salivary biomarkers for periodontal diseases. Periodontol 2000 2016;70:26-37. Pro-inflammatory chemical mediators for PD include interleukin-1 (IL-1), IL-6, tumor necrosis factor alpha, matrix metalloproteinases (MMPs), complement factors, RANKL and interferon gamma.44Cekici A, Kantarci A, Hasturk H, Van Dyke TE. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontol 2000 2014;64(1):57-80.,45Liu YC, Lerner UH, Teng YT. Cytokine responses against periodontal infection: protective and destructive roles. Periodontol 2000 2010;52:163-206.,46Steinsvoll S, Halstensen TS, Schenck K. Extensive expression of TGF-beta1 in chronically-inflamed periodontal tissue. J Clin Periodontol 1999;26:366-73.,47Garlet GP. Destructive and protective roles of cytokines in periodontitis: a re-appraisal from host defense and tissue destruction viewpoints. J Dent Res 2010;89:1349-63. Protective factors include transforming growth factor beta, tissue inhibitors of metalloproteinases, IL-4, osteoprotegerin, and IL-10.44Cekici A, Kantarci A, Hasturk H, Van Dyke TE. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontol 2000 2014;64(1):57-80.,45Liu YC, Lerner UH, Teng YT. Cytokine responses against periodontal infection: protective and destructive roles. Periodontol 2000 2010;52:163-206.,48Reis C, Costa AV, Guimarães JT, Tuna D, Braga AC, Pacheco JJ, Arosa FA, Salazar F, Cardoso EM. Clinical improvement following therapy for periodontitis: Association with a decrease in IL-1 and IL-6 Exp Ther Med. 2014;8(1):323-7. Tests and research have evaluated genetic variation associated with IL-1 overexpression.42Kim JJ, Kim CJ, Camargo PM. Salivary biomarkers in the diagnosis of periodontal diseases. J Calif Dent Assoc. 2013;41(2):119-24.
Salivary proteome information can be used to identify combinations of biomarkers for use in a single test and are believed to be more predictive of disease progression/stability than one biomarker.43Korte DL, Kinney J. Personalized medicine: an update of salivary biomarkers for periodontal diseases. Periodontol 2000 2016;70:26-37. Promising results for PD monitoring have been found for the combination of MMP-8, osteoprotegerin and macrophage inflammatory protein-1x. Additionally, the combination of MMP-8 and IL1- β as biomarkers correlates positively with BOP, AL and the percentage of sites with a PPD ≥4 mm.43Korte DL, Kinney J. Personalized medicine: an update of salivary biomarkers for periodontal diseases. Periodontol 2000 2016;70:26-37. Transcriptome research using salivary mRNA is being used to identify gene overexpression/underexpression in patients with and without periodontal disease, and in other research other biomarkers and combinations of microbial and salivary biomarkers are being investigated.19Page RC, Krall EA, Martin J, Mancl L, Garcia RI. Validity and accuracy of a risk calculator in predicting periodontal disease. J Am Dent Assoc 2002;133(5):569-76.,42Kim JJ, Kim CJ, Camargo PM. Salivary biomarkers in the diagnosis of periodontal diseases. J Calif Dent Assoc. 2013;41(2):119-24. While more research is needed, these are promising avenues for adjunctive periodontal risk assessment.
Conclusions
Accurate periodontal risk assessment aids decision-making, patient care and treatment outcomes. Validated periodontal risk assessment tools can increase the accuracy and repeatability of risk assessment and resulting reports can help educate patients. It has been reported that providing more education and research results on the use and value of these tools in patient care settings, and encouraging self-reported patient information and integrated electronic health records to help save time, could help to encourage adoption by dental professionals by removing perceived barriers to use.27Thyvalikakath T, Song M, Schleyer T. Perceptions and attitudes toward performing risk assessment for periodontal disease: a focus group exploration. BMC Oral Health 2018;18(1):90.,37 Periodontal risk assessment tools can validate clinical care protocols and health improvements, automate pre-determination of evidence-based benefits and reduce barriers to treatment acceptance.25Busby M, Chapple E, Matthews R, Chapple ILC. Practitioner evaluation of a novel online integrated oral health and risk assessment tool: a practice pilot. Br Dent J 2013;215(3):115-20.,26Delargy S, Busby M, McHugh S, Matthews R, Burke FJ. The reproducibility of the Denplan Oral Health Score (OHS) in general dental practitioners. Community Dent Health 2007;24:105-10.,38Martin J, Mills S, Foley ME. Innovative models of dental care delivery and coverage. Patient-centric dental benefits based on digital oral health risk assessment. Dent Clin N Am 2018;62:319-25. Further, risk assessment tools hold promise for assessing oral health outcomes at the patient, provider and population group level; for clinical audits; and, in the design of informed reimbursement strategies based on disease severity and outcomes.25Busby M, Chapple E, Matthews R, Chapple ILC. Practitioner evaluation of a novel online integrated oral health and risk assessment tool: a practice pilot. Br Dent J 2013;215(3):115-20.,26Delargy S, Busby M, McHugh S, Matthews R, Burke FJ. The reproducibility of the Denplan Oral Health Score (OHS) in general dental practitioners. Community Dent Health 2007;24:105-10.,38Martin J, Mills S, Foley ME. Innovative models of dental care delivery and coverage. Patient-centric dental benefits based on digital oral health risk assessment. Dent Clin N Am 2018;62:319-25.,39Mills SE. Creating a risk-based model for dental benefit design. J Dent Hyg 2015;89(Suppl 1):24-6. In the area of salivary biomarkers, promising results and concentrated research efforts are underway to identify robust biomarkers for PD and its progression. Personalized care and treatment could be enhanced in the coming years through the use of validated periodontal risk assessment tools and chairside testing for salivary biomarkers.6Bartold PM. Lifestyle and periodontitis: The emergence of personalized periodontics. Periodontol 2000 2018 Oct;78(1):7-11.,49Giannobile WV. Salivary diagnostics for periodontal diseases. J Am Dent Assoc 2012;143(Suppl 10):6S–11S.
References
- 1.Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJ, Marcenes W. Global burden of severe periodontitis in 1990–2010: A systematic review and meta-regression. J Dent Res 2014;93:1045-53.
- 2.Nazir MA. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int J Health Sci 2017;11:72–80.
- 3.Eke PI, Dye BA, Wei L, Thornton-Evans GO, Genco RJ, et al. Prevalence of periodontitis in adults in the United States: 2009 and 2010. J Dent Res 2012;91(10):914-20.
- 4.Eke PI, Wei L, Borgnakke WS, Zhang X, Lu H, McGuire LC, Genco RJ. Periodontitis prevalence in adults ≥ 65 years of age, in the USA. Periodontol 2000 2016;72(1):76-95.
- 5.Lang NP, Bartold MP. Periodontal health. J Clin Periodontol 2018;45(Suppl 20):S9-16.
- 6.Bartold PM. Lifestyle and periodontitis: The emergence of personalized periodontics. Periodontol 2000 2018 Oct;78(1):7-11.
- 7.Caton JG, Armitage G, Berglundh T, Chapple ILC, Jepsen S, Kornman KS, Mealey BL, Papapanou PN, Sanz M, Tonetti MS. A new classification scheme for periodontal and peri-implant diseases and conditions – Introduction and key changes from the 1999 classification. J Periodontol 2018;89(Suppl 1):S1-8.
- 8.American Academy of Periodontology. Statement on risk assessment. J Periodontol 2008;79:202.
- 9.World Health Organization. Risk factors. Available at: https://www.who.int/topics/risk_factors/en/.
- 10.Chapple IL, Genco R, Working Group 2 of the Joint EFP/AAP Workshop. Diabetes and periodontal diseases. Consensus report of the Joint EFP/AAP Workshop on periodontitis and systemic diseases. J Periodontol 2013;84(4):S106-12.
- 11.Albandar JM, Streckfus CF, Adesanya MR, Winn DM. Cigar, pipe, and cigarette smoking as risk factors for periodontal disease and tooth loss. J Periodontol 2000;71(12):1874-81.
- 12.Shariff JA, Ahluwalia KP, Papapanou PN. Relationship between frequent recreational cannabis (marijuana and hashish) use and periodontitis in adults in the United States: Nhanes 2011-12. J Periodontol 2017;88(3):273-80.
- 13.Hach M, Holm-Pedersen P, Adegboye A, Avlund K. The effect of alcohol consumption on periodontitis in older Danes. Int J Dent Hyg 2015;12:1-7.
- 14.Suvan JE, Finer N, D’Aiuto F. Periodontal complications with obesity. Periodontol 2000 2018;78(1):98-128.
- 15.American Dental Association. Electronic oral health risk assessment tools. SCDI White Paper No. 1074, 2013. Available at: http://www.ada.org/~/media/ADA/Science%20and%20Research/Files/ADAWhitePaperNo1074.pdf?la=en.
- 16.Scher JU, Ubeda C, Equinda M, Khanin R, Buischi Y, Viale A, Lipuma L, Attur M, Pillinger MH, Weissmann G, Littman DR, Pamer EG, Bretz WA, Abramson SB. Periodontal disease and the oral microbiota in new onset rheumatoid arthritis. Arthritis Rheum 2012;64:3083-94.
- 17.Berthelot J-M, Le Goff B. Rheumatoid arthritis and periodontal disease. Joint Bone Spine 2010;77(6):537-41.
- 18.Kurushima Y, Tsai PC, Castillo-Fernandez J, Couto Alves A, El-Sayed Moustafa JS, Le Roy C, Spector TD, Ide M, Hughes FJ, Small KS, Steves CJ, Bell JT. Epigenetic findings in periodontitis in UK twins: a cross-sectional study. Clin Epigenetics 2019;11(1):27.
- 19.Page RC, Krall EA, Martin J, Mancl L, Garcia RI. Validity and accuracy of a risk calculator in predicting periodontal disease. J Am Dent Assoc 2002;133(5):569-76.
- 20.Page RC, Martin J, Krall EA, Mancl L, Garcia R. Longitudinal validation of a risk calculator for periodontal disease. J Clin Periodontol 2003;30:819-27.
- 21.Sandberg HCH, Fors UGH. The HIDEP model--a straightforward dental health care model for prevention-based practice management. Swed Dent J 2007;31(4):171-9.
- 22.Page RC, Martin JA, Loeb CF. The Oral Health Information Suite (OHIS): Its use in the management of periodontal disease. J Dent Ed 2005;69(5):509-20.
- 23.Carrington MJ, Kok S, Jansen K, Stewart S. The Green, Amber, Red Delineation of Risk and Need (GARDIAN) management system: a pragmatic approach to optimizing heart health from primary prevention to chronic disease management. Eur J Cardiovasc Nurs 2013;12(4):337-45.
- 24.Martin JA, Page RC, Kaye EK, Hamed MT, Loeb CF. Periodontitis severity plus risk as a tooth loss predictor. J Periodontol 2009;80(2):202-9.
- 25.Busby M, Chapple E, Matthews R, Chapple ILC. Practitioner evaluation of a novel online integrated oral health and risk assessment tool: a practice pilot. Br Dent J 2013;215(3):115-20.
- 26.Delargy S, Busby M, McHugh S, Matthews R, Burke FJ. The reproducibility of the Denplan Oral Health Score (OHS) in general dental practitioners. Community Dent Health 2007;24:105-10.
- 27.Thyvalikakath T, Song M, Schleyer T. Perceptions and attitudes toward performing risk assessment for periodontal disease: a focus group exploration. BMC Oral Health 2018;18(1):90.
- 28.Lang NP, Tonetti MS. Periodontal risk assessment (PRA) for patients in supportive periodontal therapy (SPT). Oral Health Prev Dent 2003;1:7-16.
- 29.Matuliene G, Studer R, Lang NP, Schmidlin K, Pjetursson BE, Salvi GE, Brägger U, Zwahlen M. Significance of Periodontal Risk Assessment on the recurrence of periodontitis and tooth loss. J Clin Periodontol 2010;37:191-9.
- 30.Jansson H, Norderyd O. Evaluation of a periodontal risk assessment model in subjects with severe periodontitis. A 5-year retrospective study. Swed Dent J 2008;32(1):1-7.
- 31.Chandra RV. Evaluation of a novel periodontal risk assessment model in patients presenting for dental care. Oral Health Prev Dent 2007;5(1):39-48.
- 32.Leininger M, Tenenbaum H, Davideau J-L. Modified periodontal risk assessment score: long-term predictive value of treatment outcomes. A retrospective study. J Clin Periodontol 2010;37(5):427-35.
- 33.Trombelli L, Farina R, Ferrari S, Pasetti P, Calura G. Comparison between two methods for periodontal risk assessment. Minerva Stomatol 2009;58:277-87.
- 34.Persson GR, Mancl LA, Martin JA, Page RC. Assessing periodontal disease risk. J Am Dent Assoc 2003;134(5):575-82.
- 35.Martin JA, Grill AC, Matthews AG, Vena D, Thompson VP, Craig RG, Curro FA. Periodontal diagnosis affected by variation in terminology. Periodontol 2013;84:606-13.
- 36.Lang NP, Suvan JE, Tonetti MS. Risk factor assessment tools for the prevention of periodontitis progression a systematic review. J Clin Periodontol 2015;42(S16):S59-70.
- 37.Mertz E, Wides C, White J. Clinician attitudes, skills, motivations and experience following the implementation of clinical decision support tools in a large dental practice. J Evid Based Dent Pract 2017;17(1):1-12.
- 38.Martin J, Mills S, Foley ME. Innovative models of dental care delivery and coverage. Patient-centric dental benefits based on digital oral health risk assessment. Dent Clin N Am 2018;62:319-25.
- 39.Mills SE. Creating a risk-based model for dental benefit design. J Dent Hyg 2015;89(Suppl 1):24-6.
- 40.Shimazaki Y, Akifusa S, Takeshita T, Shibata Y, Doi Y, Hata J, Ninomiya T, Hirakawa Y, Kiyohara Y, Yamashita Y. Effectiveness of the salivary occult blood test as a screening method for periodontal status J Periodontol. 2011;82(4):581-7.
- 41.Reed SG, Manz M, Snipe SM, Ohshimna M, Wagner CL. Feasibility study of a salivary occult blood test to correlate with periodontal measures as indicators of periodontal inflammation in a population of pregnant women. J Oral Sci 2015;57(1): 55-8.
- 42.Kim JJ, Kim CJ, Camargo PM. Salivary biomarkers in the diagnosis of periodontal diseases. J Calif Dent Assoc. 2013;41(2):119-24.
- 43.Korte DL, Kinney J. Personalized medicine: an update of salivary biomarkers for periodontal diseases. Periodontol 2000 2016;70:26-37.
- 44.Cekici A, Kantarci A, Hasturk H, Van Dyke TE. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontol 2000 2014;64(1):57-80.
- 45.Liu YC, Lerner UH, Teng YT. Cytokine responses against periodontal infection: protective and destructive roles. Periodontol 2000 2010;52:163-206.
- 46.Steinsvoll S, Halstensen TS, Schenck K. Extensive expression of TGF-beta1 in chronically-inflamed periodontal tissue. J Clin Periodontol 1999;26:366-73.
- 47.Garlet GP. Destructive and protective roles of cytokines in periodontitis: a re-appraisal from host defense and tissue destruction viewpoints. J Dent Res 2010;89:1349-63.
- 48.Reis C, Costa AV, Guimarães JT, Tuna D, Braga AC, Pacheco JJ, Arosa FA, Salazar F, Cardoso EM. Clinical improvement following therapy for periodontitis: Association with a decrease in IL-1 and IL-6 Exp Ther Med. 2014;8(1):323-7.
- 49.Giannobile WV. Salivary diagnostics for periodontal diseases. J Am Dent Assoc 2012;143(Suppl 10):6S–11S.