

Soft Tissue Issues and Considerations in Woodwind and Brass Musicians
Among musicians, it was estimated in one review that up to 93% are affected over their lifetime by systemic health issues related to playing, especially musculoskeletal disorders.1Ackermann BJ, Driscoll T, Kenny DT. Musculoskeletal pain and injury in professional orchestral musicians in Australia. Med Probl Perform Art 2012;27(4):181-7.,2Kok LM, Huisstede BM, Voorn VM et al. The occurrence of musculoskeletal complaints among professional musicians: a systematic review. Int Arch Occup Envi 2016;8:373-97. https://doi.org/10.1007/s00420-015-1090-6.,3Brandfonbrener AG. Musculoskeletal problems of instrumental musicians. Hand Clin 2003;19(2):231-9, v-vi. doi: 10.1016/s0749-0712(02)00100-2. Studies have reported on issues related to the orofacial region, with researchers in one review concluding that temporomandibular joint disorders (TMDs), herpes simplex infections, orthodontic problems and perioral musculature issues were the most common ones.4Rodríguez-Lozano FJ, Sáez-Yuguero MR, Bermejo-Fenoll A. Orofacial problems in musicians: a review of the literature. Med Probl Perform Art 2011;26(3):150-6. In this article, we will address findings on oral and peri-oral soft tissues, the role of dental professionals, and considerations when treating wind instrumentalists. Before doing so, it is important to understand ‘embouchure’ and its importance.
Embouchure
Embouchure refers to ‘the position and use of the lips, tongue, and teeth’ when playing a wind instrument.5“Embouchure.” Merriam-Webster.com Dictionary, Merriam-Webster, https://www.merriam-webster.com/dictionary/embouchure. Contact with the mouthpiece, along with the intricate and complex movements and positions of the lips, tongue, and peri-oral musculature, determine how air reaches into the mouthpiece and, thereby, the tone, quality, articulation and volume of the music produced.6Papsin BC, Maaske LA, McGrail JS. Orbicularis oris muscle injury in brass players. Laryngoscope 1996;106(6):757-60. Functionality of the oral and peri-oral structures is key, while the manner in which wind instruments contact oral and peri-oral structures is instrument-dependent.7Fine L. Dental problems in the wind instrumentalist. Clevel Clin Q 1986;53:3-9.

Positioning of the instrument
For single-reed instruments (e.g., clarinets), a reed is attached to the inferior surface of the mouthpiece. (Figure 1) When playing single-reed instruments, the upper anterior teeth and lips rest on the mouthpiece.8Single-reed Instrument. Wikipedia. https://en.wikipedia.org/wiki/Single-reed_instrument#:~:text=The%20standard%20embouchures%20for%20single%20reed%20woodwinds%20like,top%20teeth%20rest%20on%20top%20of%20the%20mouthpiece. When playing a clarinet, the lower lip is folded over the lower incisors and the lip contacts the reed, while for the saxophone the lower teeth are usually placed directly on the reed. The flute and piccolo rest on the skin below the lower lip, with the lips configured to funnel air into the instrument. For brass instruments, the lips are compressed and contact the mouthpiece, with the teeth placed behind the lips and the upper teeth acting like a supportive scaffold.7Fine L. Dental problems in the wind instrumentalist. Clevel Clin Q 1986;53:3-9. For double-reed instruments, e.g., oboes, the upper and lower lips are pulled over the teeth, forming an intimate seal over the double reed. (Figure 2) Fine, complex movements of the orofacial musculature, including the tongue, are required to produce music with these instruments.9Double reed. Wikipedia. https://en.wikipedia.org/wiki/Double_reed#:~:text=The%20orchestral%20double%20reeds%20all%20employ%20a%20similar,from%20the%20muscles%20of%20the%20mouth%20and%20jaw. A list of wind instruments typically found in orchestras and bands and their category is included at the end of this article for reference purposes.
Figure 2. Positioning of the instrument and embouchure



Intra-oral and compressive forces
The forces applied are highest when playing brass instruments, with a reported mean force in one study of 500g.10Engelman J. Measurement of perioral pressures during playing of musical wind instruments. Am J Orthod 1965;51:856-64. In a recent study, piezoresistive sensors were used to digitally measure the forces applied during embouchure.11Clemente MP, Moreira A, Mendes J et al. Wind Instrumentalist Embouchure and the Applied Forces on the Perioral Structures. Open Dent J 2019;13(1):107-14. doi:10.2174/1874210601913010107. The maximum forces measured for the trombone, French horn, trumpet, oboe, saxophone, clarinet and bassoon were 325g, 305g, 172g, 125g 120g, 106g, and 31g, respectively. However, forces as high as 2,750g between the lips and mouthpiece have been found for professional symphony trombone players, and significantly higher forces for professional non-symphony players.12Froelich JP. Mouthpiece forces during trombone performance [dissertation]. Twin Cities, MN, Univ. of Minnesota, 1987.,13Wallace E, Klinge D, Chesky K. Musculoskeletal Pain in Trombonists Results from the UNT Trombone Health Survey. Med Probl Perform Art 2016:87-95. http://dx.doi.org/10.21091/mppa.2016.2016. These potential forces are considerably higher than that sufficient to provide for tooth movement during orthodontic treatment (generally considered to be around 50g).14Yee JA, Türk T, Elekdağ-Türk S et al. Rate of tooth movement under heavy and light continuous orthodontic forces. Am J Orthod Dentofacial Orthop 2009;136(2):150.e1-9; discussion 150-1. doi: 10.1016/j.ajodo.2009.03.026. Given the potential compressive forces and intraoral pressures exerted on the orofacial region while playing wind instruments, it should be unsurprising that playing may increase risk for orofacial injury.
Oral and Peri-oral Soft Tissue Issues
Lip pain, swollen lips and limited lip flexibility occur among instrumentalists, as well as embouchure dystonia and other issues.15Chesky K, Devroop K, Ford J. Medical Problems of Brass Instrumentalists: Prevalence Rates for Trumpet, Trombone, French Horn, and Low Brass. Med Probl Perform Art 2002;17:93-8. https://doi.org/10.21091/mppa.2002.2013.,16Slotte R. Swollen Lips From Playing Trumpet TIPS To Prevent Swelling Lips When Playing. My Best Trumpet. https://mybesttrumpet.com/swollen-lips-from-playing-trumpet-lips-swelling-when-playing-trumpet/. In one survey with 340 respondents ages 13 to 50, cheek and lip myospasms, dental problems, TMDs, gingival and tongue lesions, and wounds/ulcerations to the labial musculature were reported by 34.5%, 30.7%, 22.5%, 7.8% and 5% of respondents, respectively.17Sayegh Ghoussoub M, Ghoussoub K, Chaaya A et al. Orofacial and hearing specific problems among 340 wind instrumentalists in Lebanon. MJ Med Liban 2008;56(3):159-67. [Article in French] (Figure 3) Lengthier practice was an influencing factor.
Lip Pain and Injuries
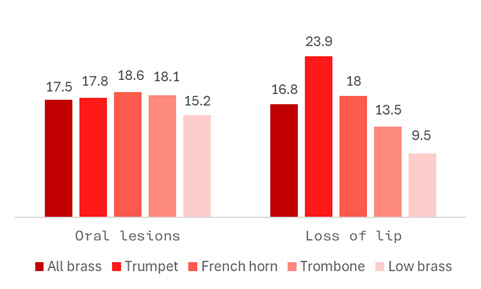
Lip pain and injuries are a common complaint, with 23% of trombone players in one survey reporting lip pain in the prior year.13Wallace E, Klinge D, Chesky K. Musculoskeletal Pain in Trombonists Results from the UNT Trombone Health Survey. Med Probl Perform Art 2016:87-95. http://dx.doi.org/10.21091/mppa.2016.2016. In an evaluation of data for more than 700 brass instrumentalists, 24% of players were found to have experienced ‘loss of lip’ (pain, fatigue, loss of control or loss of power in the lips/orofacial area).14Yee JA, Türk T, Elekdağ-Türk S et al. Rate of tooth movement under heavy and light continuous orthodontic forces. Am J Orthod Dentofacial Orthop 2009;136(2):150.e1-9; discussion 150-1. doi: 10.1016/j.ajodo.2009.03.026. Differences were observed across instrumentalists, e.g., 23.9% of trumpet players suffered loss of lip compared to 9.5% of ‘low brass’ players (baritone horn, tuba, and euphonium). In addition, 17.5% of players overall experienced oral lesions. (Figure 4)
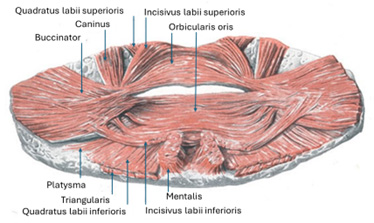
In a third study with approximately 600 brass players, 59% self-reported embouchure-related problems.18Steinmetz A, Stand A, Kornhuber M et al. From embouchure problems to embouchure dystonia?: a survey of self-reported embouchure disorders in 585 professional orchestra brass players. Int Arch Occup Environ Health 2014;87(7):783-92. doi:10.1007/s00420-013-0923-4. Lip injuries that affect embouchure include compression neuropathies, tendinitis, musician’s dystonia, ‘blowing out’ of the upper lip among brass players and injury to the orbicularis oris musculature.19Woldendorp K H, Boschma H, Boonstra AM et al. Fundamentals of Embouchure in Brass Players: Towards a Definition and Clinical Assessment. Med Probl Perform Art 2016; 31(4):232-43. https://www.jstor.org/stable/48714435. Rupture of the orbicularis oris muscle can result in pain, fatigue and an inability to play, necessitating surgical repair.6Papsin BC, Maaske LA, McGrail JS. Orbicularis oris muscle injury in brass players. Laryngoscope 1996;106(6):757-60. (Figure 5)

Louis Armstrong (Satchmo) suffered from peri-oral soft tissue issues during his career, thought until recently to be damage to the orbicularis oris muscle. However, recent research indicated that his injuries began with superficial damage to labial skin, then cracks and fissures that healed with scar tissue.20Rosset-Llobet J, Rosset-Garric Q, Grimalt R. Louis Armstrong's Lip Problems: Satchmo's Syndrome Reviewed. Med Probl Perform Art 2023;38(1):1-8. Such scar tissue is fibrotic and stiff, resulting in the need for even more force. The researchers concluded that he likely suffered from fibromatous hyperplasia.
Embouchure Dystonia
Embouchure dystonia causes loss of control of the orofacial musculature. It typically first occurs in middle age, with an inability to perform certain notes or genres, and then progresses further.21Frucht SJ, Fahn S, Greene PE et al. The natural history of embouchure dystonia. Mov Disord 2001;16(5):899-906. This condition causes individuals to experience involuntary movements of peri-oral muscles, tremors, or jaw closing and may or may not be painful. It is unfortunately difficult to treatment.
Peri-oral Skin Conditions
Dermatitis, allergic conditions, cheilitis and black dermographism have been reported among musicians.22Gambichler T, Boms S, Freitag M. Contact dermatitis and other skin conditions in instrumental musicians. BMC Dermatol 2004;4:3. doi: 10.1186/1471-5945-4-3.,23Baccouche D, Mokni M, Ben Abdelaziz A, Ben Osman-Dhahri A. Dermatological problems of musicians: a prospective study in music students. [Article in French] Annal Dermatol Vénéréol 2007;134(5:1):445-9.,24Rimmer S, Spielvogel RL. Dermatologic problems of musicians. J Am Acad Dermatol 1990;22:657-63. Flautists and brass players typically use mouthpieces that can release nickel following contact with sweat and saliva, which may result in contact dermatitis or allergic contact dermatitis, and can be associated with cheilitis.22Gambichler T, Boms S, Freitag M. Contact dermatitis and other skin conditions in instrumental musicians. BMC Dermatol 2004;4:3. doi: 10.1186/1471-5945-4-3.,23Baccouche D, Mokni M, Ben Abdelaziz A, Ben Osman-Dhahri A. Dermatological problems of musicians: a prospective study in music students. [Article in French] Annal Dermatol Vénéréol 2007;134(5:1):445-9.,25Crepy MN. Skin diseases in musicians. Eur J Dermatol 2015;25(5):375-83.,26Freeman S, Stephens R. Cheilitis: analysis of 75 cases referred to a contact dermatitis clinic. Am J Contact Dermat 1999;10(4):198-200. doi: 10.1053/AJCD01000198. Similarly, exotic woods can cause irritant contact dermatitis and allergic contact dermatitis, such as rosewood used for flutes and recorders, and Cocobolo wood and African blackwood for other instruments.22Gambichler T, Boms S, Freitag M. Contact dermatitis and other skin conditions in instrumental musicians. BMC Dermatol 2004;4:3. doi: 10.1186/1471-5945-4-3. In addition, allergic reactions to cane reeds (manufactured from a reed grass) have been reported in clarinetists and saxophonists.22Gambichler T, Boms S, Freitag M. Contact dermatitis and other skin conditions in instrumental musicians. BMC Dermatol 2004;4:3. doi: 10.1186/1471-5945-4-3.,27MacFadden JP, Ingram MJ, Rycroft RJG. Contact allergy to cane reed in a saxophonist. Contact Dermat 1992;37:117. These reactions present as cheilitis, with scaling and redness, erosions and lower lip fissures near the midline. Immediate-type allergic reactions can also occur. If allergies are suspected, the instrumentalist can be patch-tested for potential allergen(s).25Crepy MN. Skin diseases in musicians. Eur J Dermatol 2015;25(5):375-83.,28Podjasek JO, Cook-Norris RH, Richardson DM et al. Allergic contact dermatitis from exotic woods: importance of patch-testing with patient-provided samples. Dermatitis 2011;22(2):E1-6. Lastly, black dermographism of the lower lip and/or in the area between the lip and chin is reported in flautists. This discoloration can occur if a flute’s mouthpiece contains silver, and it contacts sulfur or zinc oxide.
For the conditions described above, plastic and gold-plated mouthpieces can be used instead of nickel-containing mouthpieces, instruments manufactured from materials other than exotic woods can be used, and cane reeds can be replaced with plastic polystyrene reeds.22Gambichler T, Boms S, Freitag M. Contact dermatitis and other skin conditions in instrumental musicians. BMC Dermatol 2004;4:3. doi: 10.1186/1471-5945-4-3.,25Crepy MN. Skin diseases in musicians. Eur J Dermatol 2015;25(5):375-83.,28Podjasek JO, Cook-Norris RH, Richardson DM et al. Allergic contact dermatitis from exotic woods: importance of patch-testing with patient-provided samples. Dermatitis 2011;22(2):E1-6. Individuals experiencing black dermographism should either use a non-silver mouthpiece or avoid items containing sulfur or zinc oxide (such as anti-acne lotions, some make-up powder and moisturizers).

Source: Centers for Disease Control and Prevention
Herpes labialis
Herpes labialis has been found to be more common in wind instrumentalists than non-musicians, and the lesions impact playing.29Barkvoll P, Attramadal A. Recurrent herpes labialis in a military brass band. Eur J Oral Sci 1987;95:256-8. https://doi.org/10.1111/j.1600-0722.1987.tb01838.x (Figure 6) Mechanical stress/lip trauma and emotional stress are among the triggers for herpes labialis and can be induced by playing.30Stoopler ET, Kuperstein AS, Sollecito TP. How do I Manage a Patient with Recurrent Herpes Simplex? J Can Dent Assoc 2012;78:c154. https://jcda.ca/article/c154/.
Potential for transmission of infection
Wind instruments can harbor microorganisms introduced during playing, e.g., herpes simplex, herpes zoster, hepatitis A and B, measles virus, staphylococci, and fungi.22Gambichler T, Boms S, Freitag M. Contact dermatitis and other skin conditions in instrumental musicians. BMC Dermatol 2004;4:3. doi: 10.1186/1471-5945-4-3.,31Louisiana Department of Health & Hospitals. Public Health. Infection Control and Musical Instruments, 2010. https://ldh.la.gov/assets/oph/Center-PHCH/Center-CH/infectious-epi/EpiManual/ICMusicalInstruments.pdf. ,32Gallagher S. Sharing Musical Instruments Means Sharing Germs. Tufts Now, May 2011. https://now.tufts.edu/2011/05/12/sharing-musical-instruments-means-sharing-germs. As such, loaned instruments and shared mouthpieces/reeds are potential vehicles for microbial transmission.22Gambichler T, Boms S, Freitag M. Contact dermatitis and other skin conditions in instrumental musicians. BMC Dermatol 2004;4:3. doi: 10.1186/1471-5945-4-3.,31Louisiana Department of Health & Hospitals. Public Health. Infection Control and Musical Instruments, 2010. https://ldh.la.gov/assets/oph/Center-PHCH/Center-CH/infectious-epi/EpiManual/ICMusicalInstruments.pdf. In one study of instruments used in a high school band, more than 400 bacteria and multiple fungi were found.33Academy of General Dentistry. Used woodwind and brass musical instruments harbor harmful bacteria and fungi. Dental Tribune, May 2011. https://us.dental-tribune.com/news/used-woodwind-and-brass-musical-instruments-harbor-harmful-bacteria-and-fungi/. Recommendations to reduce the risk of transmission of microorganisms include not sharing instruments (including mouthpieces) and reeds, and thoroughly drying the internal and external surfaces of wind instruments with a cloth after each use. Instruments with several parts should be disassembled before doing so, including removing reeds.34Bridges C, Mobley J. Wind Ensemble Infectious Disease Risks II A Microbiological Examination of Condensate Liquids in Woodwind Instruments. Texas Pub Health J 2016;68:6-10. Instruments and mouthpieces should also be disinfected or sterilized on a regular basis. Bleach and alcohol are not recommended, and plastics used for wind instruments, mouthpieces and reeds cannot be heat sterilized.
Implications for Dental Professionals
Dental professionals should be aware of, and understand, the range of orofacial soft tissue issues that can occur among wind instrumentalists. A second consideration is the need for an awareness of the implications and impact of poor oral health, and potential risks of dental treatment on the ability of musicians to perform and steps that can be taken. Consideration must be given to avoiding and mitigating the potential effects of dental treatment on the wind instrumentalist’s ability to perform music. These potential impacts are not theoretical, and their potential seriousness should not be underestimated. For example, Ronnie Scott, a renowned jazz saxophonist, required dental treatment in the mid-1990s that affected his embouchure, permanently impacted his ability to play, and led to depression.36Cusick J. Jazz star Ronnie Scott dropped suicide hints. December 27, 1996. https://www.independent.co.uk/news/jazz-star-ronnie-scott-dropped-suicide-hints-1316088.html.
Oral care and prevention
As with all patients, oral hygiene instruction, appropriate in-office and home preventive care should be provided. In instrumentalists experiencing dry mouth, advice is needed on how to minimize dry mouth and palliative care to relieve dry mouth (in addition to stepped-up preventive care).7Fine L. Dental problems in the wind instrumentalist. Clevel Clin Q 1986;53:3-9.
Management of soft tissue complaints
Labial pain and lesions associated with contact with teeth during playing can be reduced by smoothing incisal edges or restorations (or fixed orthodontic appliances). Vacuformed thin flexible lip guards can be used to protect labial tissues pressed against the teeth.7Fine L. Dental problems in the wind instrumentalist. Clevel Clin Q 1986;53:3-9.,35Howard JA, Lovrovich AT. Wind instruments: their interplay with orofacial structures. Med Probl Perform Art 1989;4:59-72. If embouchure dystonia is suspected, the patient should be referred to a neurologist.21Frucht SJ, Fahn S, Greene PE et al. The natural history of embouchure dystonia. Mov Disord 2001;16(5):899-906. For patients experiencing herpes labialis lesions, a one-time application of benzalkonium chloride formulation (Viroxyl) during the prodromal phase can prevent further lesion development. Treatment options for lesions until they heal include 5% acyclovir (Zovirax), 10% docosanol (Abreva, and 1% penciclivir (Denavir).30Stoopler ET, Kuperstein AS, Sollecito TP. How do I Manage a Patient with Recurrent Herpes Simplex? J Can Dent Assoc 2012;78:c154. https://jcda.ca/article/c154/. For instrumentalists who experience frequent herpes labialis lesions, prophylactic use of 5% acyclovir has been recommended.29Barkvoll P, Attramadal A. Recurrent herpes labialis in a military brass band. Eur J Oral Sci 1987;95:256-8. https://doi.org/10.1111/j.1600-0722.1987.tb01838.x As always, the reader should consult the drug prescribing information on dosage and frequency, absolute and relative contraindications, and adverse events, before prescribing or recommending any medication.
Burden of treatment and avoiding/mitigating risks
Digital scans of the dentition and occlusion can be taken pre-emptively and archived in case dental treatment is required in the future – e.g., direct or indirect restorations, anterior tooth replacement, or more complex treatment. Archived scans serve to inform treatment that maintains the oral and peri-oral architecture, increasing the likelihood of compatibility with the patient’s pre-existing embouchure. If digital scans are not an option, accurate polyether or polyvinylsiloxane impressions can be taken, and study models created and stored. Additionally, should treatment be needed, diagnostic wax-ups and provisionals allows for determination of the acceptability of the proposed result for embouchure, and adjustments if needed.
The instrumentalist’s playing schedule (practice and concerts), downtime and preferences are factors in the timing and type of dental care, requiring careful and collaborative consideration. Sufficient post-surgical healing time is essential, given the burden of intra-oral pressure and compressive forces among wind instrumentalists. If tooth replacement is required, implant-supported restorations provide a stable structure, and, should full extractions and a full prosthesis be required, implant-retained options provide for stability. An embouchure denture is an alternative option, used only for playing, and is fabricated with an instrument-specific bite opening and interlocking inclined planes.7Fine L. Dental problems in the wind instrumentalist. Clevel Clin Q 1986;53:3-9.,34Bridges C, Mobley J. Wind Ensemble Infectious Disease Risks II A Microbiological Examination of Condensate Liquids in Woodwind Instruments. Texas Pub Health J 2016;68:6-10.,37Porter MM. Dental problems in wind instrument playing. 6. Single reed instruments – The embouchure denture. Br Dent J 1968;124:34-6. Creating a layer of soft compressible acrylic that fits over a denture to re-create the individual instrumentalist’s embouchure has also been recommended.7Fine L. Dental problems in the wind instrumentalist. Clevel Clin Q 1986;53:3-9.,37Porter MM. Dental problems in wind instrument playing. 6. Single reed instruments – The embouchure denture. Br Dent J 1968;124:34-6. Lastly, should a parent or instrumentalist inquire about the risk of microbial transmission, they can be advised to avoid sharing instruments, mouthpieces and reeds. They can also be informed that cleaning cloths and solutions are available that are specifically manufactured for use on musical instruments and reeds, and to ask the instrument (and reed) manufacturer/distributer or supplier for instructions on regular cleaning and on disinfection (or sterilization).
Conclusions
Oral and peri-oral structures are critical to a functional embouchure, and the maintenance of oral health is a key factor. It is also clear from the literature that occupation-related risks to oral health exist for wind instrumentalists, and that treatment can impact the individual’s ability to play. As an avid musician, the author of this course has personally known wind instrumentalists who experienced oral and peri-oral issues, including in one case a blown lip. Recently, surveys on music-related pain and injuries among musicians have been enhanced and new ones developed for improved evaluation of pain, impact on playing, monitoring and, with sufficient information on predictive factors, prevention and treatment improved.13Wallace E, Klinge D, Chesky K. Musculoskeletal Pain in Trombonists Results from the UNT Trombone Health Survey. Med Probl Perform Art 2016:87-95. http://dx.doi.org/10.21091/mppa.2016.2016.,38Zão A, Altenmüller E, Azevedo L. Development and Initial Validation of the First Questionnaire to Evaluate Performance-related Pain Among Musicians with Different Backgrounds: Performance-related Pain Among Musicians Questionnaire (PPAM). J Occup Rehabil 2024;34(1):216-37. doi: 10.1007/s10926-023-10130-6. ,39Berque P, Gray H, McFadyen A. Playing-Related Musculoskeletal Problems Among Professional Orchestra Musicians in Scotland: A Prevalence Study Using a Validated Instrument, the Musculoskeletal Pain Intensity and Interference Questionnaire for Musicians (MPIIQM) Med Probl Perform Art 2016;31(2):78-86. Dental professionals need to understand the unique demands and needs of wind instrumentalists in order to be able to treat and support them by providing advice and preventive care, treatment and pre-emptively keeping scans and records for future use should they be needed. Wind instrumentalists can be referred to specialists for dental care as indicated or requested.
References
- 1.Ackermann BJ, Driscoll T, Kenny DT. Musculoskeletal pain and injury in professional orchestral musicians in Australia. Med Probl Perform Art 2012;27(4):181-7.
- 2.Kok LM, Huisstede BM, Voorn VM et al. The occurrence of musculoskeletal complaints among professional musicians: a systematic review. Int Arch Occup Envi 2016;8:373-97. https://doi.org/10.1007/s00420-015-1090-6.
- 3.Brandfonbrener AG. Musculoskeletal problems of instrumental musicians. Hand Clin 2003;19(2):231-9, v-vi. doi: 10.1016/s0749-0712(02)00100-2.
- 4.Rodríguez-Lozano FJ, Sáez-Yuguero MR, Bermejo-Fenoll A. Orofacial problems in musicians: a review of the literature. Med Probl Perform Art 2011;26(3):150-6.
- 5.“Embouchure.” Merriam-Webster.com Dictionary, Merriam-Webster, https://www.merriam-webster.com/dictionary/embouchure.
- 6.Papsin BC, Maaske LA, McGrail JS. Orbicularis oris muscle injury in brass players. Laryngoscope 1996;106(6):757-60.
- 7.Fine L. Dental problems in the wind instrumentalist. Clevel Clin Q 1986;53:3-9.
- 8.Single-reed Instrument. Wikipedia. https://en.wikipedia.org/wiki/Single-reed_instrument#:~:text=The%20standard%20embouchures%20for%20single%20reed%20woodwinds%20like,top%20teeth%20rest%20on%20top%20of%20the%20mouthpiece.
- 9.Double reed. Wikipedia. https://en.wikipedia.org/wiki/Double_reed#:~:text=The%20orchestral%20double%20reeds%20all%20employ%20a%20similar,from%20the%20muscles%20of%20the%20mouth%20and%20jaw.
- 10.Engelman J. Measurement of perioral pressures during playing of musical wind instruments. Am J Orthod 1965;51:856-64.
- 11.Clemente MP, Moreira A, Mendes J et al. Wind Instrumentalist Embouchure and the Applied Forces on the Perioral Structures. Open Dent J 2019;13(1):107-14. doi:10.2174/1874210601913010107.
- 12.Froelich JP. Mouthpiece forces during trombone performance [dissertation]. Twin Cities, MN, Univ. of Minnesota, 1987.
- 13.Wallace E, Klinge D, Chesky K. Musculoskeletal Pain in Trombonists Results from the UNT Trombone Health Survey. Med Probl Perform Art 2016:87-95. http://dx.doi.org/10.21091/mppa.2016.2016.
- 14.Yee JA, Türk T, Elekdağ-Türk S et al. Rate of tooth movement under heavy and light continuous orthodontic forces. Am J Orthod Dentofacial Orthop 2009;136(2):150.e1-9; discussion 150-1. doi: 10.1016/j.ajodo.2009.03.026.
- 15.Chesky K, Devroop K, Ford J. Medical Problems of Brass Instrumentalists: Prevalence Rates for Trumpet, Trombone, French Horn, and Low Brass. Med Probl Perform Art 2002;17:93-8. https://doi.org/10.21091/mppa.2002.2013.
- 16.Slotte R. Swollen Lips From Playing Trumpet TIPS To Prevent Swelling Lips When Playing. My Best Trumpet. https://mybesttrumpet.com/swollen-lips-from-playing-trumpet-lips-swelling-when-playing-trumpet/.
- 17.Sayegh Ghoussoub M, Ghoussoub K, Chaaya A et al. Orofacial and hearing specific problems among 340 wind instrumentalists in Lebanon. MJ Med Liban 2008;56(3):159-67. [Article in French]
- 18.Steinmetz A, Stand A, Kornhuber M et al. From embouchure problems to embouchure dystonia?: a survey of self-reported embouchure disorders in 585 professional orchestra brass players. Int Arch Occup Environ Health 2014;87(7):783-92. doi:10.1007/s00420-013-0923-4.
- 19.Woldendorp K H, Boschma H, Boonstra AM et al. Fundamentals of Embouchure in Brass Players: Towards a Definition and Clinical Assessment. Med Probl Perform Art 2016; 31(4):232-43. https://www.jstor.org/stable/48714435.
- 20.Rosset-Llobet J, Rosset-Garric Q, Grimalt R. Louis Armstrong's Lip Problems: Satchmo's Syndrome Reviewed. Med Probl Perform Art 2023;38(1):1-8.
- 21.Frucht SJ, Fahn S, Greene PE et al. The natural history of embouchure dystonia. Mov Disord 2001;16(5):899-906.
- 22.Gambichler T, Boms S, Freitag M. Contact dermatitis and other skin conditions in instrumental musicians. BMC Dermatol 2004;4:3. doi: 10.1186/1471-5945-4-3.
- 23.Baccouche D, Mokni M, Ben Abdelaziz A, Ben Osman-Dhahri A. Dermatological problems of musicians: a prospective study in music students. [Article in French] Annal Dermatol Vénéréol 2007;134(5:1):445-9.
- 24.Rimmer S, Spielvogel RL. Dermatologic problems of musicians. J Am Acad Dermatol 1990;22:657-63.
- 25.Crepy MN. Skin diseases in musicians. Eur J Dermatol 2015;25(5):375-83.
- 26.Freeman S, Stephens R. Cheilitis: analysis of 75 cases referred to a contact dermatitis clinic. Am J Contact Dermat 1999;10(4):198-200. doi: 10.1053/AJCD01000198.
- 27.MacFadden JP, Ingram MJ, Rycroft RJG. Contact allergy to cane reed in a saxophonist. Contact Dermat 1992;37:117.
- 28.Podjasek JO, Cook-Norris RH, Richardson DM et al. Allergic contact dermatitis from exotic woods: importance of patch-testing with patient-provided samples. Dermatitis 2011;22(2):E1-6.
- 29.Barkvoll P, Attramadal A. Recurrent herpes labialis in a military brass band. Eur J Oral Sci 1987;95:256-8. https://doi.org/10.1111/j.1600-0722.1987.tb01838.x
- 30.Stoopler ET, Kuperstein AS, Sollecito TP. How do I Manage a Patient with Recurrent Herpes Simplex? J Can Dent Assoc 2012;78:c154. https://jcda.ca/article/c154/.
- 31.Louisiana Department of Health & Hospitals. Public Health. Infection Control and Musical Instruments, 2010. https://ldh.la.gov/assets/oph/Center-PHCH/Center-CH/infectious-epi/EpiManual/ICMusicalInstruments.pdf.
- 32.Gallagher S. Sharing Musical Instruments Means Sharing Germs. Tufts Now, May 2011. https://now.tufts.edu/2011/05/12/sharing-musical-instruments-means-sharing-germs.
- 33.Academy of General Dentistry. Used woodwind and brass musical instruments harbor harmful bacteria and fungi. Dental Tribune, May 2011. https://us.dental-tribune.com/news/used-woodwind-and-brass-musical-instruments-harbor-harmful-bacteria-and-fungi/.
- 34.Bridges C, Mobley J. Wind Ensemble Infectious Disease Risks II A Microbiological Examination of Condensate Liquids in Woodwind Instruments. Texas Pub Health J 2016;68:6-10.
- 35.Howard JA, Lovrovich AT. Wind instruments: their interplay with orofacial structures. Med Probl Perform Art 1989;4:59-72.
- 36.Cusick J. Jazz star Ronnie Scott dropped suicide hints. December 27, 1996. https://www.independent.co.uk/news/jazz-star-ronnie-scott-dropped-suicide-hints-1316088.html.
- 37.Porter MM. Dental problems in wind instrument playing. 6. Single reed instruments – The embouchure denture. Br Dent J 1968;124:34-6.
- 38.Zão A, Altenmüller E, Azevedo L. Development and Initial Validation of the First Questionnaire to Evaluate Performance-related Pain Among Musicians with Different Backgrounds: Performance-related Pain Among Musicians Questionnaire (PPAM). J Occup Rehabil 2024;34(1):216-37. doi: 10.1007/s10926-023-10130-6.
- 39.Berque P, Gray H, McFadyen A. Playing-Related Musculoskeletal Problems Among Professional Orchestra Musicians in Scotland: A Prevalence Study Using a Validated Instrument, the Musculoskeletal Pain Intensity and Interference Questionnaire for Musicians (MPIIQM) Med Probl Perform Art 2016;31(2):78-86.
Resource
| Woodwind instruments | |
|---|---|
| No reed |
|
| Double reed |
|
| Single reed |
|
| Brass Instruments | |
| Trumpet, bugle, cornet, flugelhorn, euphonium, French horn, mellophone, trombone, tuba, contrabass tuba. | |