

Patient information
- Male, age 72
- Chief concern: “I want to replace my missing front tooth as soon as possible, I don’t feel like myself and I don’t smile these days”
- Patient at UBC since 2014
Medical history
- Hypertension since 2017
- Atopic dermatitis (eczema)
- Allergic rhinitis (hay fever)
- Allergic to pollen and lactose
- Medications:
- Telmisartan (Micardis) 80 mg 1x/day
- Antihistamine Cetirizine Hydrochloride (Reactine) PRN
- Non-smoker
- Non-drinker
- Family history of colon cancer (mother)
- Colonoscopy examination done with no significant findings
- ASA 2
- Most recent vitals:
- Blood pressure reading: 108/ 67 mmHg
- Pulse: 63 BPM
- Respiratory rate: 15
- Temperature: 36.6 C
Dental history
- History of lost tooth due to trauma (tooth 11 lost at 10 years old)
- History of fear of dental treatment
- Oral hygiene:
- Brushes 2x/day with a manual toothbrush for about a minute using fluoride toothpaste, using sweeping motion side by side
- Flosses 1x/day at night using string dental floss, but does not clean under the bridge because patient states it is too difficult
- Notices bleeding of the gums almost every time when brushing
- Does not use any mouth rinse or high-fluoride toothpaste
- The patient is not happy with his smile and the appearance of his teeth
- History of multiple cavities, fillings, root canals, crowns, bridges
- Does not wear his existing lower partial removable denture due to discomfort
- No sensitivity to cold, hot, sweets, or pressure
- No oral habits including clenching, bruxing, grinding
Cultural and socioeconomic factors
- During his childhood, grew up very poor and stated that he did not get enough nutrients including calcium and milk
- Lower socioeconomic status and family support were associated with a higher likelihood of infrequent toothbrushing and high sugar consumption1Gazzaz AZ, Carpiano RM, Aleksejuniene J. Socioeconomic status, social support, and oral health-risk behaviors in Canadian adolescents. J Public Health Dent. 2021 Dec;81(4):316-326. doi: 10.1111/jphd.12478. Epub 2021 Sep 30. PMID: 34590718.
- When he broke his front tooth when he was 10, no one had interest and he could not go visit the dentist and the gap naturally closed together
- Both the experience and education in dental health during childhood were found to significantly influence lifelong oral health
- The patient lives alone as his wife passed away and his children live separately because “they have their own life and families”
- A systematic review showed a positive association between marital status and social isolation with poor oral health-related quality of life among the elderly2Baniasadi K, Armoon B, Higgs P, Bayat AH, Mohammadi Gharehghani MA, Hemmat M, Fakhri Y, Mohammadi R, Fattah Moghaddam L, Schroth RJ. The Association of Oral Health Status and socio-economic determinants with Oral Health-Related Quality of Life among the elderly: A systematic review and meta-analysis. Int J Dent Hyg. 2021 May;19(2):153-165. doi: 10.1111/idh.12489. Epub 2021 Feb 14. PMID: 33523593.
- “Now I have all the money but it’s too late to gain my oral health back because I have already lost some teeth”
- With a history of fear of dental treatment, a study showed that negative experiences at a dentist may result in a poorer attitude toward oral hygiene3Mueller M, Schorle S, Vach K, Hartmann A, Zeeck A, Schlueter N. Relationship between dental experiences, oral hygiene education and self-reported oral hygiene behaviour. PLoS One. 2022 Feb 24;17(2):e0264306. doi: 10.1371/journal.pone.0264306. PMID: 35202439; PMCID: PMC8870456.
- There was a lack of awareness of preventative measures that can be implemented to stop caries progression and stabilize the periodontal disease
- Patient usually does not seek dental treatment first until a student contacts him to book an appointment for an examination or cleaning, even though he has some discomfort and pain in his teeth
- The patient is usually told what treatment needs to be done and believe those would solve all the problems, however, long-term maintainability goals were not addressed and achieved
- Due to the patient’s hay fever and chronic coughing, he sometimes does not feel comfortable coming to the dental office because others may see him as sick and spreading a cold, therefore he mostly avoids visiting during allergy season
- The patient also wears dental gloves throughout the whole appointments
- When patient was asked what his long-term goal was, patient stated “to stay healthy and prevent early death”
- The patient stays active and exercises regularly to stay fit, however, there is a lack of dietary knowledge and education that may negatively impact his physical and oral health
- The patient usually eats out or buys take-outs and whenever he is watching TV he eats a lot of junk food that is convenient and drinks a lot of juice
- Also, when the patient needs to take medication at night due to eczema, he eats some food but does not always brush after because he “gets lazy”
Caries risk assessment
- Elevators
- Frequent snack between main meals = yes
- Medications or other chemicals potentially disturbing saliva = yes
- Telmisartan and reactine are both known to have side effects of dry mouth
- Visible plaque greater than 50% of the surfaces of 50% of the teeth = yes
- Unusually rough or pitted dental surfaces = yes
- Orthodontic appliances = no
- Removable partial denture = yes
- Indicators
- Clinically white (demineralized) spot lesion on smooth surface = yes
- Cavity visible clinically or radiographically = yes
- Dental restorations made in the previous three years = yes
- Reducers
- Residence in community with fluoridated water supply = no
- Uses fluoridated toothpaste at least once daily = yes
- Uses high concentration of fluoridated toothpaste daily = no
- Uses fluoridated mouth rinse at least 3x/ week in the previous 6 months = no
- Fluoride varnish applied to teeth in previous 6 months = no
- Uses xylitol gum or lozenge daily in previous 6 months = no
- Uses calcium phosphate toothpaste daily in previous 6 months = no
- Patient is high risk for caries
- High risk for recurrent caries
- Higher risk especially for patients with poor oral hygiene
- Reducers are not adequate to manage the risk
Extra-oral examination
- 1x1mm black nodule, elevated, defined borders, at the front of the left ear, asymptomatic
- Nasal septum deviated to the left
- TMJ: deviation to the right when opening with bilateral click, asymptomatic
- No significant findings for: neck, masseter muscles, lymph nodes, other facial areas
Intra-oral examination
- Bilateral linea alba on buccal mucosa
- Scalloped tongue
- Occlusal examination
- Right Class I molar (left side cannot be determined due to missing 36)
- 0% OB
- 0mm OJ
- Upper midline shifted to the right
- No significant findings for: floor of the mouth, palate, tongue, oropharynx
Restorative charting
- Deformities and conditions:
- Open contact: 14/15, 41/ 31, 31/ 32
- Tight contact: 12/ 13
- Open margin: 15M
- Defective restoration: 12L
- Crowding, malpositions:
- Rotations: 12, 37, 32
- Lingually tipped: 12
- Crossbite: 12/ 42, 13/ 43, 14/44
- Attrition: 21, 23, 43, 34, 37
- Erosion: 37O
- Moderate recurrent caries: 15DB, 13MV, 12MV, 21V, 23MV, 27B, 48MB
- Extensive recurrent caries: 14MD
- Arrested caries: 44D, 26L, 27L

Working cast

Intraoral photograph
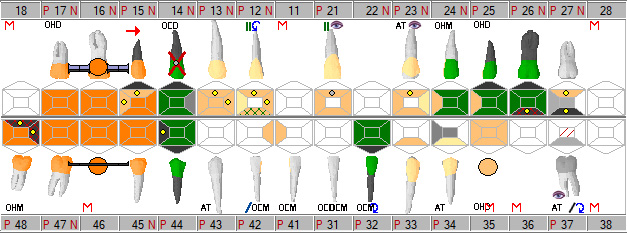
Periodontal charting
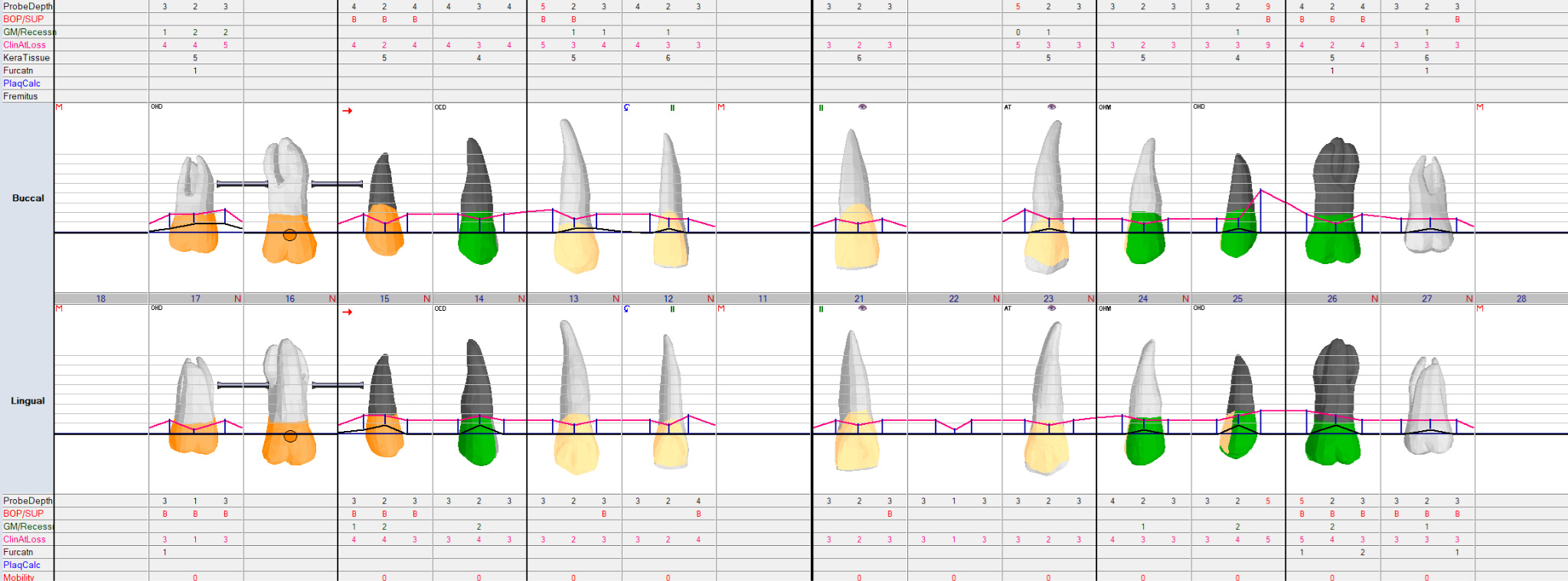
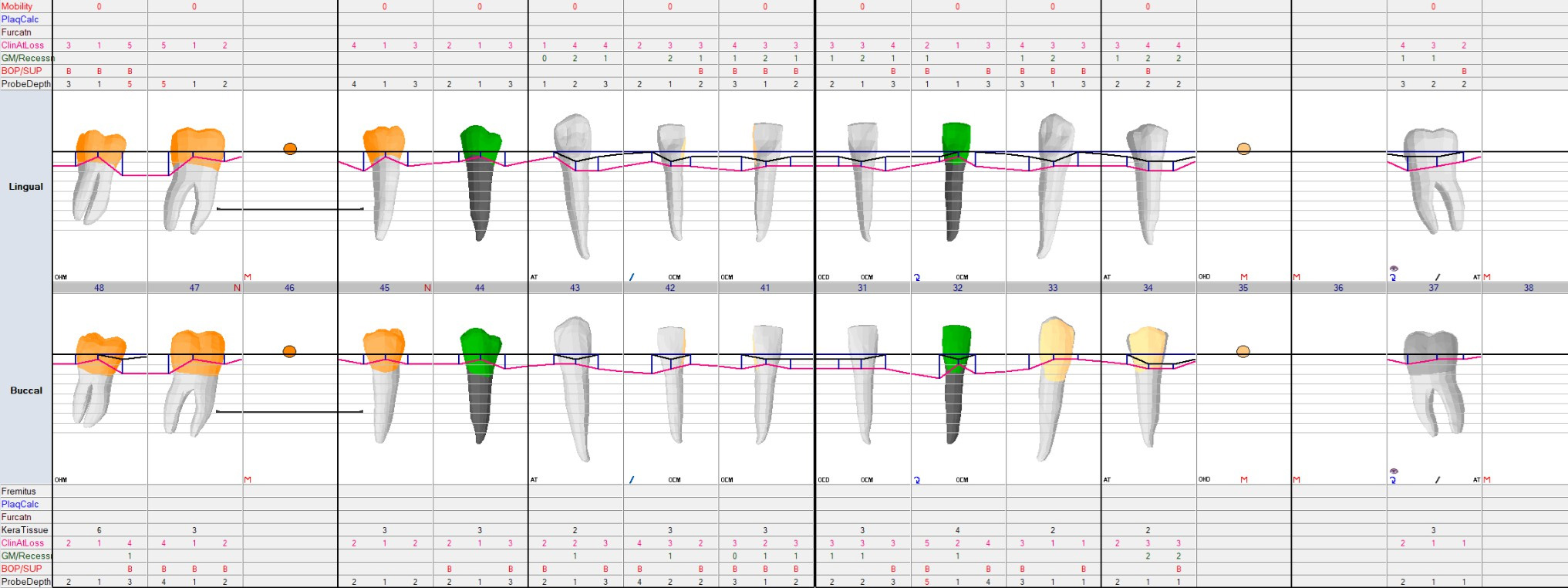
- Probing depth
- 4mm: 15, 14, 12, 24, 26, 45, 42
- 5mm: 13, 32, 47, 48
- 10mm: 25DB
- Recession of 2mm: 17, 15, 14, 25, 26, 32, 33, 31, 41, 42
- Furcation:
- Class I - 17B/ DL, 26B/ ML, 27B/ DL
- Class II - 26DL
- Lack of minimal KT (<2mm): 33/ 43/ 43
- No occlusal trauma/ mobility
- OH effectiveness: 10%
- BOP: 79.2%
- Plaque/ calculus:
- Generalized moderate plaque accumulation, especially along gingival margin
- Localized calculus interproximal of molars and lingual of lower anterior
- Color:
- Marginal gingiva: generalized red
- Interdental gingiva: redness between 33/32, 41/42, 42/43, 43/44, 44-46
- Attached gingiva: generalized pink
- Contour: generalized scalloped except loss of scalloping interdental gingiva from 42-32
- Consistency:
- Marginal gingiva: generalized firm, except bogginess at 14B, 37BL, 35B, 34B, 32-42B, 44-48B
- Interdental gingiva: generalized firm except bogginess from 42-32
- Shape:
- Marginal gingiva: generalized round
- Interdental gingiva: open embrasure on 13/12, 23/24, 34/33, 32-43
- Surface texture: generalized stippling
X-rays

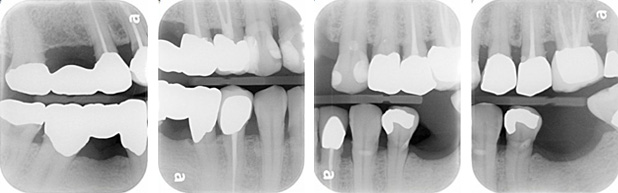
3PAs + 4BWs
- Interproximal calculus: 17M, 15D, 25MD, 26D, 33M, 37M, 47D, 48M
- Generalized mild horizontal bone loss
- Widening of PDL space: 35M/D
- 1:1 crown to root ratio: 26
- Apical radiolucency: 25
- Short root filling: 25
Diagnosis
- Periodontitis Localized Stage II Grade B Progression: 13, 23, 32 47, 48
- Primary etiology: biofilm
- Secondary etiology: difficult access under bridge, defective interproximal restorations, crowding/ malpositions, tight/ light contact
- Poor oral hygiene
- Missing 11/ unacceptable esthetics
- Moderate recurrent caries: 15DB, 13MV, 12MV, 21V, 23MV, 27B, 48MB
- Extensive recurrent caries: 14MD
- 25 Previously root canal treated with symptomatic apical periodontitis
Treatment plan
- Phase 1
- 22 Flipper denture
- Full initial therapy for periodontitis
- Oral hygiene instructions
- Fluoride varnish
- Re-evaluation after 6-8 weeks
- Direct restorations: 15DB, 13MV, 12MV, 21V, 23MV, 27B, 48MB
- 6 monthly application of 38% silver diamine fluoride: 44D, 26L, 27L
- 14 Extraction
- 25 re-RCT
- Phase 2
- 14 and 22 definitive tx options: Implant, bridge, or maxillary partial denture
- 25 ACC
- Phase 3
- SPT every 3-4 months
- Caries management
- Periodic caries risk assessment
- Perio recall examination every 12 months
- Assess frequency of recalls based on patient’s outcome
Specific preventive treatment
-
- 38% Silver Diamine Fluoride application underneath the posterior bridges and crowns
- As a result of its fluoride content, showed efficacy in managing root caries in elderly as an “off-label use”4Li R, Lo EC, Liu BY, Wong MC, Chu CH. Randomized clinical trial on arresting dental root caries through silver diammine fluoride applications in community-dwelling elders. J Dent 2016.
- Preventative measure for posterior surfaces where it is difficult for the patient to clean adequately even with proper oral hygiene methods
- Fluoride varnish application during SPTs and annual periodontal examinations
- ADA recommends using 5% sodium fluoride varnish as a preventive treatment for caries in all age groups5Research Services and Scientific Information, ADA Library & Archives. (2023, June 14). Fluoride: Topical and systemic supplements. American Dental Association. https://www.ada.org/en/resources/research/science-and-research-institute/oral-health-topics/fluori de-topical-and-systemic-supplements,6Baik A, Alamoudi N, El-Housseiny A, Altuwirqi A. Fluoride Varnishes for Preventing Occlusal Dental Caries: A Review. Dent J (Basel). 2021 Jun 3;9(6):64. doi: 10.3390/dj9060064. PMID: 34204978; PMCID: PMC8229232./li>
- ICDAS Foundation recommends patients to receive fluoride varnish by dental professionals up to 4 times a year for high caries risk patients7Carey CM. Focus on fluorides: update on the use of fluoride for the prevention of dental caries. J Evid Based Dent Pract. 2014 Jun;14 Suppl:95-102. doi: 10.1016/j.jebdp.2014.02.004. Epub 2014 Feb 13. PMID: 24929594; PMCID: PMC4058575.
- More regular SPTs
- Schedule patient for SPT every 3-4 months, and make appointments ahead of time so that the patient does not have to wait until a student reaches out
- According to the American Academy of Periodontology, during SPT, the dentist should also re-evaluate periodontal status and assess caries risk and the need for further treatment in sites showing recurrent or persistent diseases8Manresa C, Sanz-Miralles EC, Twigg J, Bravo M. Supportive periodontal therapy (SPT) for maintaining the dentition in adults treated for periodontitis. Cochrane Database Syst Rev. 2018 Jan 1;1(1):CD009376. doi: 10.1002/14651858.CD009376.pub2. PMID: 29291254; PMCID: PMC6491071.
- Diet
- Diet survey for a personalized and comprehensive assessment of caries prevention
- According to the ADA, patients with high caries risk should be instructed to reduce of amount and frequency of carbohydrate consumption9Research Services and Scientific Information, ADA Library & Archives. (2023b, July 18). Caries risk assessment and management. American Dental Association. https://www.ada.org/en/resources/research/science-and-research-institute/oral-health-topics/caries
-risk-assessment-and-management
- Try to have 3 meals a day that are focused on healthy protein, whole grains, vegetables and fruits and less in sugar and minimize snacking between meals
- When he needs to have food at night, advised him to have healthier snacks that are cariostatic including cheese, milk, and high-fiber vegetables
- Advised to rinse with water after drinking acidic drinks including juice and coffee or chew xylitol gum to stimulate salivary flow
- Oral hygiene instructions
- Brush 2 times a day using high-fluoride toothpaste (5,000 ppm F) for 2 minutes
- Brush gently at 45 angle to the gum line, to ensure that the bristles enter the gingival sulcus and use a gentle circular movement
- Showed proper Modified bass brushing technique with Mr. Smiley
- Used disclosing solution to highlight areas of plaque accumulation and high amount of calculus accumulation on lingual surfaces where patient states he was not brushing well
- Floss 1x/day using a C-shaped technique
- Care not to use too much force which can cause gingival trauma as there is gingival inflammation
- Different tools to clean under the bridge:
- Proxabrush/ interdental brush
- Super floss
- Waterpik flossers
- Floss threader requires a bit more effort, the patient might be less inclined to use it compared to simpler methods
- Showed how to use each floss with patient holding the mirror, advised patient to try all of them and see which one is more comfortable and convenient
- Tongue brush
- Replace toothbrush every 3-4 months
- Made sure patient understood the instructions with teach-back method
- 38% Silver Diamine Fluoride application underneath the posterior bridges and crowns

Oral hygiene methods

Disclosing solution
- Product recommendations based on the patient’s periodontal status:
- Colgate Periogard toothpaste
- Reduce gum bleeding, inflammation, plaque build-up, sensitivity
- Soft bristle toothbrush to prevent aggressive brushing and bleeding of gums
- Periogard SF Ultra soft gum protection toothbrush
- ADA recommends using a soft bristle toothbrush as this is most effective in removing plaque and debris without damaging your teeth and gums
- Colgate sensitive pro-relief mouthwash 1x/day
- Colgate Periogard toothpaste
- Instructions on how to clean the denture:
- Remove denture from the mouth and rinse with warm water
- With a denture brush, gently brush your denture using a non-abrasive denture cleaner to remove plaque and debris then rinse again with warm water
- Soak the denture in denture-cleaning solution overnight and do not let the denture dry out which may cause it to become more brittle
- Do not wear the denture when sleeping
Patient outcomes
- Beginning from a thorough comprehensive examination to developing a personalized treatment plan that not only addresses his current dental needs but also setting SMART goals for the long term management of his oral health was an imperative journey for myself and the patient
- Although patient has been a patient for a long time at UBC, his long history of caries and frequent restorative procedures was an indication of inadequate caries management including oral hygiene practices, preventative treatment and low sugar diet
- The first treatment that was offered was making of his flipper denture as he was psychologically distressed without his front tooth which negatively affected his quality of life

Delivery of flipper denture- During these appointments, I was able to build rapport with the patient and get to know him personally which aided in creating a personalized treatment plan
- It was important to actively listen to why it has been difficult to keep up with good oral hygiene and come up with solutions that work for him in the long term
- Every risk factor for caries including poor oral hygiene, infrequent cleaning by dental professionals and high sugar consumption was discussed with the patient
- Once the patient was satisfied with the flipper denture and denture hygiene instructions were given, I visually demonstrated proper brushing techniques with dental care model and large toothbrush used for educational purposes
- Disclosing solution was used to show the patient the area of high plaque and calculus accumulation and the patient was surprised because even though he brushed before coming to the appointment, there were a lot of “pink spots”
- Visual aids were much more effective in educating the patient about oral hygiene instructions and effectiveness of his brushing method and patient said these would help him remember what was emphasized
- During scaling and root planing, there was a lot of bleeding as the gums were inflamed and heavy subgingival calculus was difficult to remove
- Few areas with deep pockets and subgingival calculus had to be anesthetized for patient comfort and through debridement
- Took two appointments for cleaning and in every appointment oral hygiene instructions were re-emphasized
- Overall, patient was highly satisfied with the educational information that was presented to him and became more motivated to change his habits to build oral health
- During the re-evaluation stage 6 weeks after the completion of debridement, patient had decreased probing depth, BOP, and increased oral hygiene effectiveness
- The patient stated that he has been using Proxabrush to clean underneath the bridge because it is the quickest and easiest
- He has also been drinking more water and chewing xylitol gums once in a while and feels his mouth is less dry than before
- Once phase I is completed, need to make sure that his periodontal state is stabilized before moving on to phase 2, which the patient understood
- Advised the patient that he needs to be more active in visiting dental offices and calling the office when he is due for a cleaning or when he has dental pain rather than waiting
- The most valuable lessons I have gained through this patient interaction:
- Involving patients in the decision making process allows them to participate actively in managing their oral health while improving their compliance and chance of successful treatment outcomes such as giving the patient a few options of methods of flossing under the bridge and allowing the patient to determine what is most beneficial and efficient
- The importance of preventative education about oral diseases and considering patient’s personal socioeconomic and cultural factors that can create barriers to maintaining oral health
- Building achievable goals with close up follow-up and monitoring of periodontal status and oral hygiene effectiveness with implementing different strategies
References
- 1.Gazzaz AZ, Carpiano RM, Aleksejuniene J. Socioeconomic status, social support, and oral health-risk behaviors in Canadian adolescents. J Public Health Dent. 2021 Dec;81(4):316-326. doi: 10.1111/jphd.12478. Epub 2021 Sep 30. PMID: 34590718.
- 2.Baniasadi K, Armoon B, Higgs P, Bayat AH, Mohammadi Gharehghani MA, Hemmat M, Fakhri Y, Mohammadi R, Fattah Moghaddam L, Schroth RJ. The Association of Oral Health Status and socio-economic determinants with Oral Health-Related Quality of Life among the elderly: A systematic review and meta-analysis. Int J Dent Hyg. 2021 May;19(2):153-165. doi: 10.1111/idh.12489. Epub 2021 Feb 14. PMID: 33523593.
- 3.Mueller M, Schorle S, Vach K, Hartmann A, Zeeck A, Schlueter N. Relationship between dental experiences, oral hygiene education and self-reported oral hygiene behaviour. PLoS One. 2022 Feb 24;17(2):e0264306. doi: 10.1371/journal.pone.0264306. PMID: 35202439; PMCID: PMC8870456.
- 4.Li R, Lo EC, Liu BY, Wong MC, Chu CH. Randomized clinical trial on arresting dental root caries through silver diammine fluoride applications in community-dwelling elders. J Dent 2016.
- 5.Research Services and Scientific Information, ADA Library & Archives. (2023, June 14). Fluoride: Topical and systemic supplements. American Dental Association. https://www.ada.org/en/resources/research/science-and-research-institute/oral-health-topics/fluori de-topical-and-systemic-supplements
- 6.Baik A, Alamoudi N, El-Housseiny A, Altuwirqi A. Fluoride Varnishes for Preventing Occlusal Dental Caries: A Review. Dent J (Basel). 2021 Jun 3;9(6):64. doi: 10.3390/dj9060064. PMID: 34204978; PMCID: PMC8229232.
- 7.Carey CM. Focus on fluorides: update on the use of fluoride for the prevention of dental caries. J Evid Based Dent Pract. 2014 Jun;14 Suppl:95-102. doi: 10.1016/j.jebdp.2014.02.004. Epub 2014 Feb 13. PMID: 24929594; PMCID: PMC4058575.
- 8.Manresa C, Sanz-Miralles EC, Twigg J, Bravo M. Supportive periodontal therapy (SPT) for maintaining the dentition in adults treated for periodontitis. Cochrane Database Syst Rev. 2018 Jan 1;1(1):CD009376. doi: 10.1002/14651858.CD009376.pub2. PMID: 29291254; PMCID: PMC6491071.
- 9.Research Services and Scientific Information, ADA Library & Archives. (2023b, July 18). Caries risk assessment and management. American Dental Association. https://www.ada.org/en/resources/research/science-and-research-institute/oral-health-topics/caries
-risk-assessment-and-management