

Introduction of Patient
Age and sex: 67-year-old, Male
Initial evaluation: October 27, 2023
Chief Complaint: “My teeth feel sticky and I want a cleaning”
Medical and Dental History
Medical History:
Cardiovascular: Arrhythmia (diagnosed in 1988), currently stable and not taking medications. He does not have hypertension. His blood pressure ranged from 116/72 - 128/86 at his last three appointments.
Central nervous system: Epilepsy (diagnosed in 1996) with episodes of simple partial seizures. His last seizure was in 2008 and is currently stable. Furthermore, the patient had a spinal cord injury in 1995, leading to compression of the spine and loss of mobility. The patient is now using a wheelchair permanently, as he cannot move his lower extremities.
Cancer: Lymphoma (diagnosed in 1988) treated by chemotherapy. He is currently still in remission and stable.
Musculoskeletal: Osteoarthritis in the upper extremities (diagnosed in 1999). He is unable to perform tasks requiring manual dexterity, such as toothbrushing and basic hygiene.
Gastrointestinal: Stomach ulcers (diagnosed in 2008) with no complications and is currently stable.
Allergies: No known allergies.
Summary of medical stability: All these conditions are stable and followed closely by his general practitioner. Due to his complex medical history, he has a personal support worker (PSW) who assists him with his daily living.
Medications:
1) Gabapentin 400 mg qd po and
2) Baclofen 40 mg qd po for epilepsy and nerve pain.
3) Losec 50 mg qd po for stomach ulcers.
Exercise:
The patient does not exercise due to osteoarthritis, loss of mobility in the lower extremities, and being bound to a wheelchair.
Diet:
The patient drinks sugared coffee/tea three times in between meals, fruit juice twice in between meals, and sweetened baked goods (doughnuts and cookies) once in between meals each day. Sugary beverages are consumed over a long duration (1-2 hours). The patient has well-balanced meals from all food groups provided to him by his PSW.
Dental History:
Dental Hygiene: The patient has osteoarthritis and cannot perform oral hygiene on himself. At the first appointment, he revealed he has a PSW that brushes for him using a manual toothbrush with Crest toothpaste 0.454% Stannous fluoride (1100 ppm fluoride) twice daily (morning before breakfast and before bedtime). No other fluoridated products are used at home. He consumes fluoridated tap water and does not use mouthwash. Fluoride varnish has been applied to his teeth at scaling and root planing (SRP) appointments. Currently, he has only been getting SRP once a year as a preventative procedure. His latest SRP was in October 2023 when I first saw the patient. During his last SRP appointment, there was heavy generalized plaque and supragingival calculus, moderate generalized subgingival calculus, and bleeding on probing (BOP) localized to the mandibular anterior teeth. The gingiva was red and inflamed throughout the mouth. The interproximal areas and gingival third of the teeth were often missed during his at-home oral hygiene regimen. The patient states the PSW brushes with horizontal strokes for less than 30 seconds each day. The patient states that he gets flossed every other day or every 3-4 days, but this did not correspond to what was seen clinically. He appeared motivated to attain better oral hygiene, but he states his PSW is not motivated to brush his teeth for longer durations and is reluctant to provide him with oral hygiene (OH) unless he requests for it daily. The patient has no family history of oral cancer, has never smoked, does not consume alcohol, does not use chewing tobacco, and does not excessively expose himself to the sun.
Appointment History: The patient has been a patient at the University of Toronto dental clinic since 2004 and generally sees the dentist once a year. In October 2023, he was transferred to me as his primary student provider.
Socioeconomic and Cultural Factors
Family and social history: The patient revealed that he immigrated to Toronto, Canada from a small town in Italy in 1984. Growing up in a small Italian town, he stated he did not have access to fluoridated water. Instead, he only started consuming fluoridated water when he moved to Toronto. He currently lives alone and does not have any family members or relatives in Canada. He further reveals that he is socially isolated with a lack of a support network. He spends the majority of the day alone in his house watching television. He stated that oral hygiene was not his priority, as he does not have any aesthetic demands of his teeth in a social setting. He mentioned some symptoms of major depressive disorder but was never formally diagnosed with a psychiatric illness.
Work and financial history: In Canada, he used to work full-time until he was diagnosed with lymphoma in 1988, for which he had to take time off work and receive treatment. He was successfully treated and returned to work until he had a spinal cord injury in 1995, which led to his loss of mobility. He has been receiving disability benefits from the government. Finances are a limiting factor in seeking dental care, he disclosed. The dental benefits he has are inadequate for his needs and he requires time to save up for dental procedures. In the past, he has had to forgo preventative SRP and restorative treatment from private practice due to financial reasons. Although he receives a steady income from the government, he states that it is inadequate and he can only afford to see the dentist when necessary.
Cultural and educational history: Growing up in a small Italian town, the patient stated that his parents worked in the agricultural industry and did not enforce any educational requirements on him. He stated that he finished secondary school but did not pursue further education. His parents did not have a strong educational background either. In school and at home, he was never taught how to properly take care of his oral health. Thus, he stated that his dental knowledge was low. The culture of his Italian town was primarily focused on agriculture and farming. He stated that it was always a busy 10-12 hour work day and he did not have time to focus on anything other than work and basic health needs, such as eating and sleeping. He stated that the busy work culture was reinforced throughout his community, rather than developing work-life balance. When asked about his adolescent dental history in Italy, he stated that he had been to the dentist less than 15 times. He does not recall what had been done or if they provided oral hygiene instruction (OHI) to him. In the Italian culture, he discussed his frequent consumption of dairy products and sugary foods. He stated that he would drink milk throughout the day, eat cheese regularly, and snack on Italian sweets. He remembers his adolescent meals to consist primarily of refined carbohydrates, such as bread and pasta. Ultimately, I concluded that he has had a high caries risk from a young age based on his cariogenic diet, snacking habits, and cultural/educational/social background.
Extra-Oral & Intra-Oral Examination
Facial type: Orthognathic
Profile: Straight
Lip Competence: Competent
Nasolabial angle and Labiomental fold: WNL
Symmetry: Chin deviated to the left
Angle’s Molar Classification: Class III malocclusion on both sides
Crossbites: None
Overbite: 30%
Overjet: 3 mm
Midline: Mandibular midline shifted 2 mm to the left. Maxillary midline is coincident with the facial midline.
Missing: 18, 24, 25, 26, 28, 37
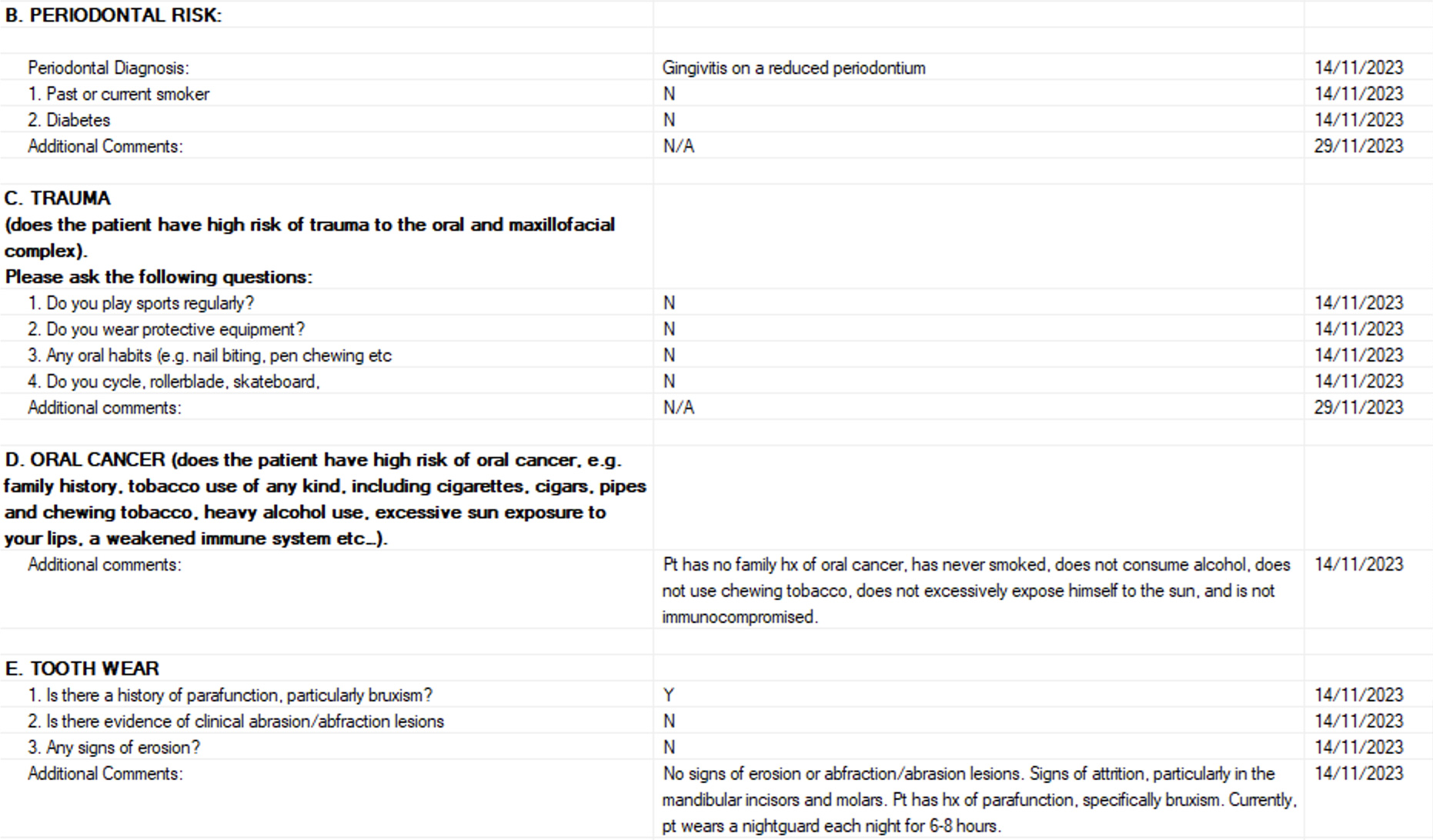
Habits: The patient is a bruxer and attrition can be seen particularly in the mandibular anterior teeth. He wears a nightguard each night for 6-8 hours.
Patient Intraoral Photographs
-

- Frontal view
-

- Maxilla
-
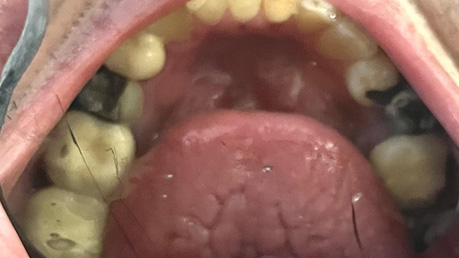
- Mandible
Dental Examination
Carious Lesions: 12MV, 13DV, 14MOV, 25O, 31V, 42MV, 45V
Patient Odontogram
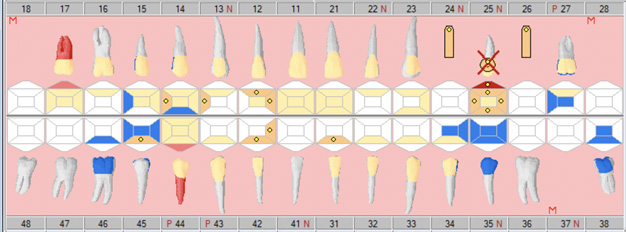
Legend
Blue: Amalgam restoration
Red: Caries
Yellow: Composite restoration
Beige: Glass Ionomer restoration
Tooth #25: Initially planned for extraction, but has instead been endodontically-treated.
Rectangles at tooth #24 and #26: Implant
Yellow dot: Planned restoration
M: Missing
Periodontal Condition and Periodontal Charting
Periodontal condition: Localized BOP in the mandibular anterior teeth. No recession, mobility, furcation, suppuration, or minimal attached width. Pocket depths are generally 2-4 mm, with clinical attachment loss of 5 mm and 6 mm at teeth #27 and #44.
Periodontal diagnosis: Gingivitis on a reduced periodontium
Gingival phenotype: Thin Scalloped
Implant health: Health at implant sites #24 and #26 without bone loss
Gingival Score: 2
Reference:
0 = Normal gingiva
1 = Mild inflammation (slight change in colour, slight edema, no bleeding on probing)
2 = Moderate inflammation: redness, edema, bleeding on probing
3 = Severe inflammation: marked redness and edema, tendency to spontaneous bleeding, ulceration
Full mouth periodontal charting recorded October 27, 2023:
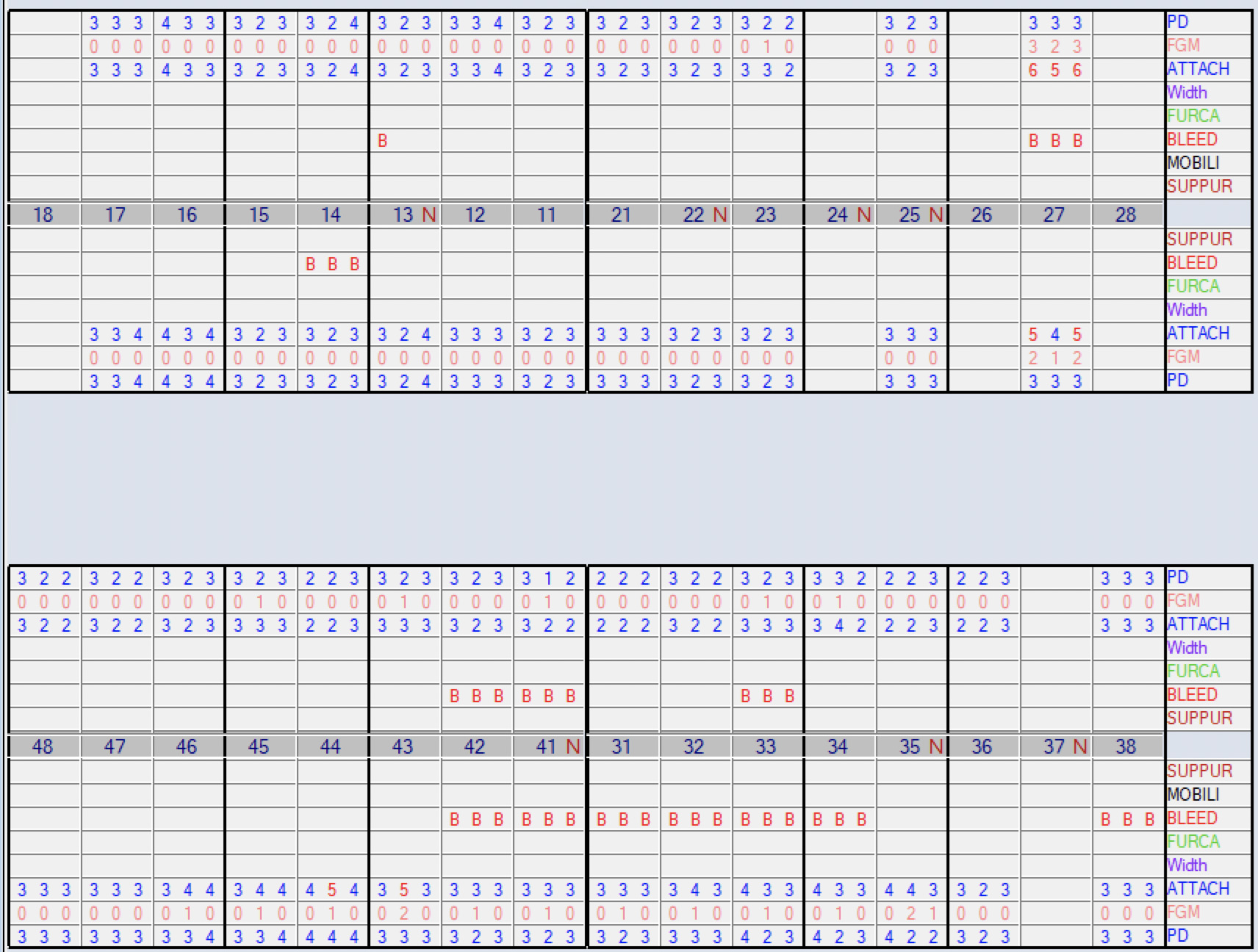
Legend:
PD: Probing depth
FGM: Free gingival margin
ATTACH: Clinical attachment level/loss
Width: Minimal attached gingiva
FURCA: Furcation
BLEED: Bleeding on probing
MOBILI: Mobility
SUPPUR: Suppuration
Plaque
Plaque score: 56%
Reference ranges:
- Thoroughly clean mouth (0 – 6%)
- Acceptable plaque score (7-21%)
- Oral hygiene needs improvement (22-100%)
My patient has a plaque score of 56%, which places him in the category of “Oral Hygiene Needs Improvement”.
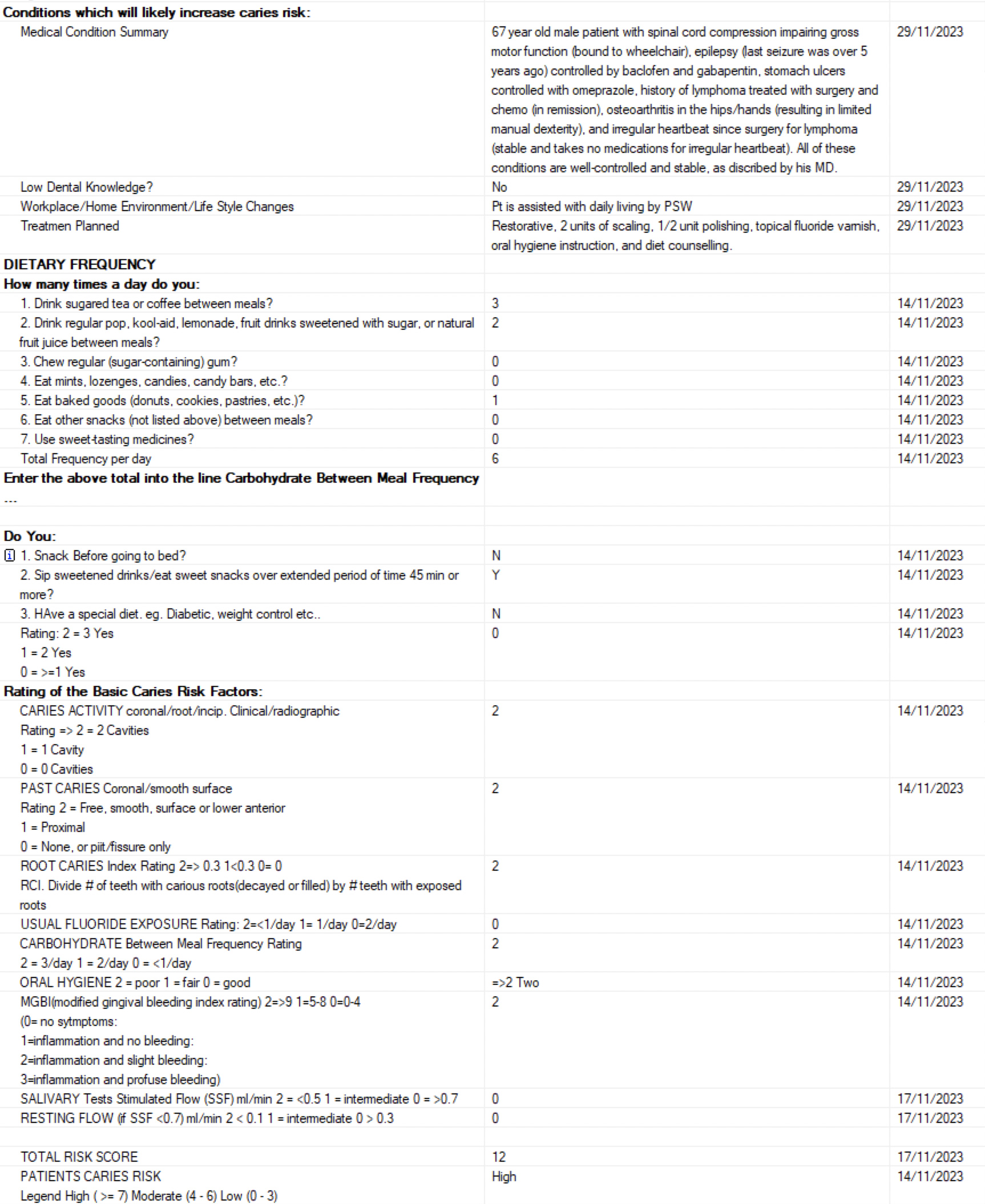
Risk Assessment
This is the risk assessment used at the University of Toronto Faculty of Dentistry. According to this assessment, the patient is currently at high risk based on his at-home oral hygiene routine, dietary habits, and clinical assessment.
Note: Salivary tests are no longer being conducted at the faculty, so the score of “0” assigned is not representative of his true salivary flow.
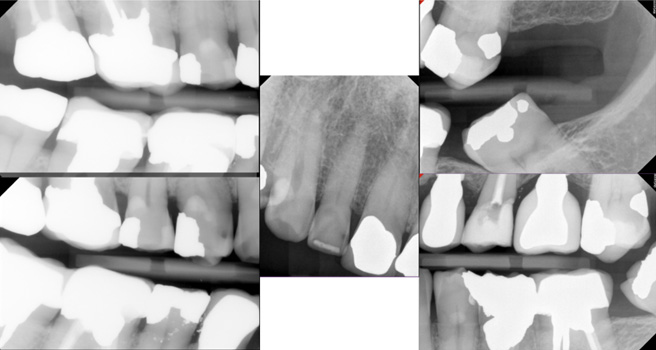
Radiographs
Patient-Specific Modifiers and Patient-Specific Treatment Objectives
Patient-specific modifiers:
- The patient relies on the Toronto Transit Commission’s wheelchair services to attend appointments. When he is unable to schedule wheelchair transport services, he is unable to come to appointments.
- Poor manual dexterity due to osteoarthritis leading to his complete reliance on his PSW for oral hygiene.
- Financial concerns: the patient is not employed due to disability and relies on government dental benefits. The patient is unable to afford all the necessary treatments presented to him.
- The patient had been on several medications causing xerostomia throughout his lifetime, including cardiovascular and CNS medications.
Patient-specific Treatment Objectives:
- Address the patient’s chief complaint
- Motivate the patient to seek more regular dental care
- Remove caries and preserve pulpal vitality when possible
- Reduce the risk of caries and periodontal disease
- Establish and maintain a healthy periodontium
- Establish a thorough oral hygiene routine with his PSW
Major Factors leading to Dental Disease Risk
- Numerous past caries, heavily restored dentition, and current caries (observed clinically and radiographically). In fact, all of his teeth have been restored except for the 36, 41, 47, and 48.
- Frequent consumption of sugary food and drinks in between meals
- Physical disability leading to his inability to perform OH by himself
- Inadequate OH provided by his PSW, leading to heavy generalized plaque and calculus buildup
- Decreased salivary flow as a side effect of medications (i.e., Baclofen and Gabapentin) and advanced age
- Infrequent SRP and professional fluoride application (only once a year) despite his high caries risk
Proposed Treatment and the Impact of the Proposed Treatment
| Treatment | Impact of Proposed Treatment |
|---|---|
| Scaling and Root Planing every 4 months | Remove calculus and plaque (containing cariogenic bacteria) from teeth to prevent future caries.1Lamont T, Worthington HV, Clarkson JE, Beirne PV. Routine scale and polish for periodontal health in adults. Cochrane Database Syst Rev. 2018 Dec 27;12(12):CD004625. doi: 10.1002/14651858.CD004625.pub5. PMID: 30590875; PMCID: PMC6516960.
Identify areas of plaque accumulation and new/recurrent canes, and provide timely restorative treatment when needed to prevent further decay and periodontal destruction. |
| Reviewing oral hygiene instruction at each appointment | Inform the patient of what adequate brushing and flossing entail so he can assess his PSW's oral hygiene technique and advise them on how to improve.
Reinforce the importance of caries/periodontitis prevention and motivate him to reduce his risk. |
| Professional fluoride application in-office and use of high-fluoride toothpaste at home (Colgate PreviDent 5000 ppm Fluoride) | Fluoride will promote remineralization and prevent demineralization of tooth structure.2Medjedovic E, Medjedovic S, Deljo D, Sukalo A. IMPACT OF FLUORIDE ON DENTAL HEALTH QUALITY. Mater Sociomed. 2015 Dec;27(6):395-8. doi: 10.5455/msm.2015.27.395-398. PMID: 26889098; PMCID: PMC4733546
Fluoride has antibacterial effects; it gets incorporated into the tooth structure to protect against acid attacks and makes cariogenic bacteria less capable of producing acid from carbohydrates.2Medjedovic E, Medjedovic S, Deljo D, Sukalo A. IMPACT OF FLUORIDE ON DENTAL HEALTH QUALITY. Mater Sociomed. 2015 Dec;27(6):395-8. doi: 10.5455/msm.2015.27.395-398. PMID: 26889098; PMCID: PMC4733546,3Nassar Y, Brizuela M. The Role of Fluoride on Caries Prevention. [Updated 2023 Mar 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK587342/ |
| Restoring carious lesions | Restoring carious lesions will remove decay and eliminate cavitations that act as bacterial traps. Restorations can prolong the lifespan of the tooth and make the tooth cleanseable.4Warreth A. Dental Caries and Its Management. Int J Dent. 2023 Jan 3;2023:9365845. doi: 10.1155/2023/9365845. PMID: 36636170; PMCID: PMC9831703. Resin-Modified Glass Ionomer (RMGI) restorations are planned for further fluoride release. For example, the 31V, 42MV, and 45V are decided to be filled with RMGI based on the “Evidence-Based Clinical Practice Guideline on Restorative Treatments for Caries Lesions” and “Restorative Treatments for Caries Lesions Clinical Practice Guideline (2023)” by the American Dental Association.5American Dental Association (2023). Evidence-Based Clinical Practice Guideline on Restorative Treatments for Caries Lesions: A Report from the American Dental Association.,6Dhar V, Pilcher L, Fontana M, González-Cabezas C, Keels MA, Mascarenhas AK, Nascimento M, Platt JA, Sabino GJ, Slayton R, Tinanoff N, Young DA, Zero DT, Pahlke S, Urquhart O, O'Brien KK, Carrasco-Labra A. Evidence-based clinical practice guideline on restorative treatments for caries lesions: A report from the American Dental Association. J Am Dent Assoc. 2023 Jul;154(7):551-566.e51. doi: 10.1016/j.adaj.2023.04.011. PMID: 37380250. |
| Reassessing risk every 4 months | Monitor if his risk has decreased (such as decreased frequency of sugary food/drink consumption) or if the patient needs further compliance aids.
Be on high alert to identify if the patient acquires any new risk factors and help guide the patient into reducing them. |
| Diet counselling at every appointment | Reducing the frequency of consumption of sugary foods/drinks will reduce the number of acid attacks on the patient's teeth and subsequent demineralization.7Tungare S, Paranjpe AG. Diet and Nutrition to Prevent Dental Problems. [Updated 2023 Jul 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534248/ |
| Discussing the use of Xylitol gum at home: 1 or 2 pieces of xylitol-containing gum, 3-5 times a day | Xylitol is an anti-cariogenic agent since it can inhibit the carbohydrate metabolism in different oral micro-organisms. It helps reduce tooth decay by reducing Strep. mutans levels in plaque and saliva, and reduce the level of lactic acid produced by these bacteria.8Janakiram C, Deepan Kumar CV, Joseph J. Xylitol in preventing dental caries: A systematic review and meta-analyses. J Nat Sci Biol Med. 2017 Jan-Jun;8(1):16-21. doi: 10.4103/0976-9668.198344. PMID: 28250669; PMCID: PMC5320817.
Chewing gum will also stimulate salivary flow to enhance protection against caries.8Janakiram C, Deepan Kumar CV, Joseph J. Xylitol in preventing dental caries: A systematic review and meta-analyses. J Nat Sci Biol Med. 2017 Jan-Jun;8(1):16-21. doi: 10.4103/0976-9668.198344. PMID: 28250669; PMCID: PMC5320817.,9Mickenautsch S, Leal SC, Yengopal V, Bezerra AC, Cruvinel V. Sugar-free chewing gum and dental caries: a systematic review. J Appl Oral Sci. 2007 Apr;15(2):83-8. doi: 10.1590/s1678-77572007000200002. PMID: 19089107; PMCID: PMC4327235. |
Summary of How the Treatment Plan Addresses Risk Factors and Meets Patient-Specific Treatment Objectives
| Objective | Treatment | Risk Factor(s) Targeted |
|---|---|---|
| Address the patient’s chief complaint of having “sticky teeth” due to plaque
Motivate the patient to seek more regular care Reduce the risk of periodontal disease Establish and maintain a healthy periodontium |
Maintain regular hygiene appointments: SRP every 4 months
SRP allows for the mechanical removal of plaque10Smiley CJ, Tracy SL, Abt E, Michalowicz BS, John MT, Gunsolley J, Cobb CM, Rossmann J, Harrel SK, Forrest JL, Hujoel PP, Noraian KW, Greenwell H, Frantsve-Hawley J, Estrich C, Hanson N. Evidence-based clinical practice guideline on the nonsurgical treatment of chronic periodontitis by means of scaling and root planing with or without adjuncts. J Am Dent Assoc. 2015 Jul;146(7):525-35. doi: 10.1016/j.adaj.2015.01.026. PMID: 26113100., leading to less “sticky teeth”, which will motivate him to continue seeking regular dental care Periodontal recall every 4 months to monitor periodontal health These treatments and recall intervals were set based on the American Dental Association’s “Nonsurgical Treatment of Chronic Periodontitis Clinical Practice Guideline (2015)”.10Smiley CJ, Tracy SL, Abt E, Michalowicz BS, John MT, Gunsolley J, Cobb CM, Rossmann J, Harrel SK, Forrest JL, Hujoel PP, Noraian KW, Greenwell H, Frantsve-Hawley J, Estrich C, Hanson N. Evidence-based clinical practice guideline on the nonsurgical treatment of chronic periodontitis by means of scaling and root planing with or without adjuncts. J Am Dent Assoc. 2015 Jul;146(7):525-35. doi: 10.1016/j.adaj.2015.01.026. PMID: 26113100. |
Heavy generalized plaque buildup
Infrequent SRP |
| Address the patient’s chief complaint of having “sticky teeth” due to plaque
Reduce the risk of caries and periodontal disease Establish a thorough oral hygiene routine |
Reinforce OHI at every appointment:
The use of PreviDent and 0.05% NaF daily (225 ppm) have been recommended to the patient based on the American Dental Association’s “Professionally-Applied and Prescription-Strength, Home-Use Topical Fluoride Agents for Caries Prevention Clinical Practice Guideline (2013)”.11Weyant RJ, Tracy SL, Anselmo TT, Beltrán-Aguilar ED, Donly KJ, Frese WA, Hujoel PP, Iafolla T, Kohn W, Kumar J, Levy SM, Tinanoff N, Wright JT, Zero D, Aravamudhan K, Frantsve-Hawley J, Meyer DM; American Dental Association Council on Scientific Affairs Expert Panel on Topical Fluoride Caries Preventive Agents. Topical fluoride for caries prevention: executive summary of the updated clinical recommendations and supporting systematic review. J Am Dent Assoc. 2013 Nov;144(11):1279-91. doi: 10.14219/jada.archive.2013.0057. Erratum in: J Am Dent Assoc. 2013 Dec;144(12):1335. Dosage error in article text. PMID: 24177407; PMCID: PMC4581720.
Thorough plaque control at home will reduce his feeling of “sticky teeth”, which will further motivate him to maintain adequate OH on a daily basis |
Physical disability leading to his inability to perform OH by himself
Inadequate OH provided by his PSW, leading to heavy generalized plaque and calculus buildup |
| Reduce the risk of caries | Professional Fluoride application: Fluoride Varnish 5% NaF (Duraflor) or APF 1.23% to be used at SRP appointments every 4 months11Weyant RJ, Tracy SL, Anselmo TT, Beltrán-Aguilar ED, Donly KJ, Frese WA, Hujoel PP, Iafolla T, Kohn W, Kumar J, Levy SM, Tinanoff N, Wright JT, Zero D, Aravamudhan K, Frantsve-Hawley J, Meyer DM; American Dental Association Council on Scientific Affairs Expert Panel on Topical Fluoride Caries Preventive Agents. Topical fluoride for caries prevention: executive summary of the updated clinical recommendations and supporting systematic review. J Am Dent Assoc. 2013 Nov;144(11):1279-91. doi: 10.14219/jada.archive.2013.0057. Erratum in: J Am Dent Assoc. 2013 Dec;144(12):1335. Dosage error in article text. PMID: 24177407; PMCID: PMC4581720.
The use of 5% NaF fluoride varnish has been recommended by the American Dental Association’s “Professionally-Applied and Prescription-Strength, Home-Use Topical Fluoride Agents for Caries Prevention Clinical Practice Guideline (2013)”.11Weyant RJ, Tracy SL, Anselmo TT, Beltrán-Aguilar ED, Donly KJ, Frese WA, Hujoel PP, Iafolla T, Kohn W, Kumar J, Levy SM, Tinanoff N, Wright JT, Zero D, Aravamudhan K, Frantsve-Hawley J, Meyer DM; American Dental Association Council on Scientific Affairs Expert Panel on Topical Fluoride Caries Preventive Agents. Topical fluoride for caries prevention: executive summary of the updated clinical recommendations and supporting systematic review. J Am Dent Assoc. 2013 Nov;144(11):1279-91. doi: 10.14219/jada.archive.2013.0057. Erratum in: J Am Dent Assoc. 2013 Dec;144(12):1335. Dosage error in article text. PMID: 24177407; PMCID: PMC4581720. |
Current infrequent professional fluoride application |
| Remove caries and preserve pulpal vitality when possible
Reduce the risk of caries |
Restore caries with composite resin and resin-modified glass ionomer (RMGI) for long-term fluoride release
The choice of composite resin and RMGI were based on the guidelines set by the American Dental Association’s “Restorative Treatments for Caries Lesions Clinical Practice Guideline (2023)”.5American Dental Association (2023). Evidence-Based Clinical Practice Guideline on Restorative Treatments for Caries Lesions: A Report from the American Dental Association.,6Dhar V, Pilcher L, Fontana M, González-Cabezas C, Keels MA, Mascarenhas AK, Nascimento M, Platt JA, Sabino GJ, Slayton R, Tinanoff N, Young DA, Zero DT, Pahlke S, Urquhart O, O'Brien KK, Carrasco-Labra A. Evidence-based clinical practice guideline on restorative treatments for caries lesions: A report from the American Dental Association. J Am Dent Assoc. 2023 Jul;154(7):551-566.e51. doi: 10.1016/j.adaj.2023.04.011. PMID: 37380250. |
|
| Reduce the risk of caries | Diet Counselling
|
Frequent consumption of sugary food and drinks between meals |
| Reduce the risk of caries | Promote the use of xylitol gum: 1 or 2 pieces of xylitol-containing gum, 3-5 times a day.12Rethman MP, Beltrán-Aguilar ED, Billings RJ, Hujoel PP, Katz BP, Milgrom P, Sohn W, Stamm JW, Watson G, Wolff M, Wright JT, Zero D, Aravamudhan K, Frantsve-Hawley J, Meyer DM; American Dental Association Council on Scientific Affairs Expert Panel on Nonfluoride Caries-Preventive Agents. Nonfluoride caries-preventive agents: executive summary of evidence-based clinical recommendations. J Am Dent Assoc. 2011 Sep;142(9):1065-1071. doi: 10.14219/jada.archive.2011.0329. PMID: 21987836.
This recommendation was based on the American Dental Association’s “Non-fluoride Caries Preventive Agents Guideline (2011)”.12Rethman MP, Beltrán-Aguilar ED, Billings RJ, Hujoel PP, Katz BP, Milgrom P, Sohn W, Stamm JW, Watson G, Wolff M, Wright JT, Zero D, Aravamudhan K, Frantsve-Hawley J, Meyer DM; American Dental Association Council on Scientific Affairs Expert Panel on Nonfluoride Caries-Preventive Agents. Nonfluoride caries-preventive agents: executive summary of evidence-based clinical recommendations. J Am Dent Assoc. 2011 Sep;142(9):1065-1071. doi: 10.14219/jada.archive.2011.0329. PMID: 21987836. |
Decreased salivary flow as a side effect of medications (specifically Baclofen and Gabapentin) and advanced age |
Note: These preventative measures were recommended based on guidelines by the American Dental Association, peer-reviewed articles on dental disease prevention, and lectures from the University of Toronto, Faculty of Dentistry.
Execution of the Treatment Plan
Appointment # 1 October 27, 2023
- Address Chief Complaint
- Periodontal therapy: 1) Initial periodontal exam, 2) scaling and root planing, 3) polishing, and 4) fluoride varnish 5% NaF (Duraflor) application
- OHI
- Diet Counselling
Official notes from the appointment:
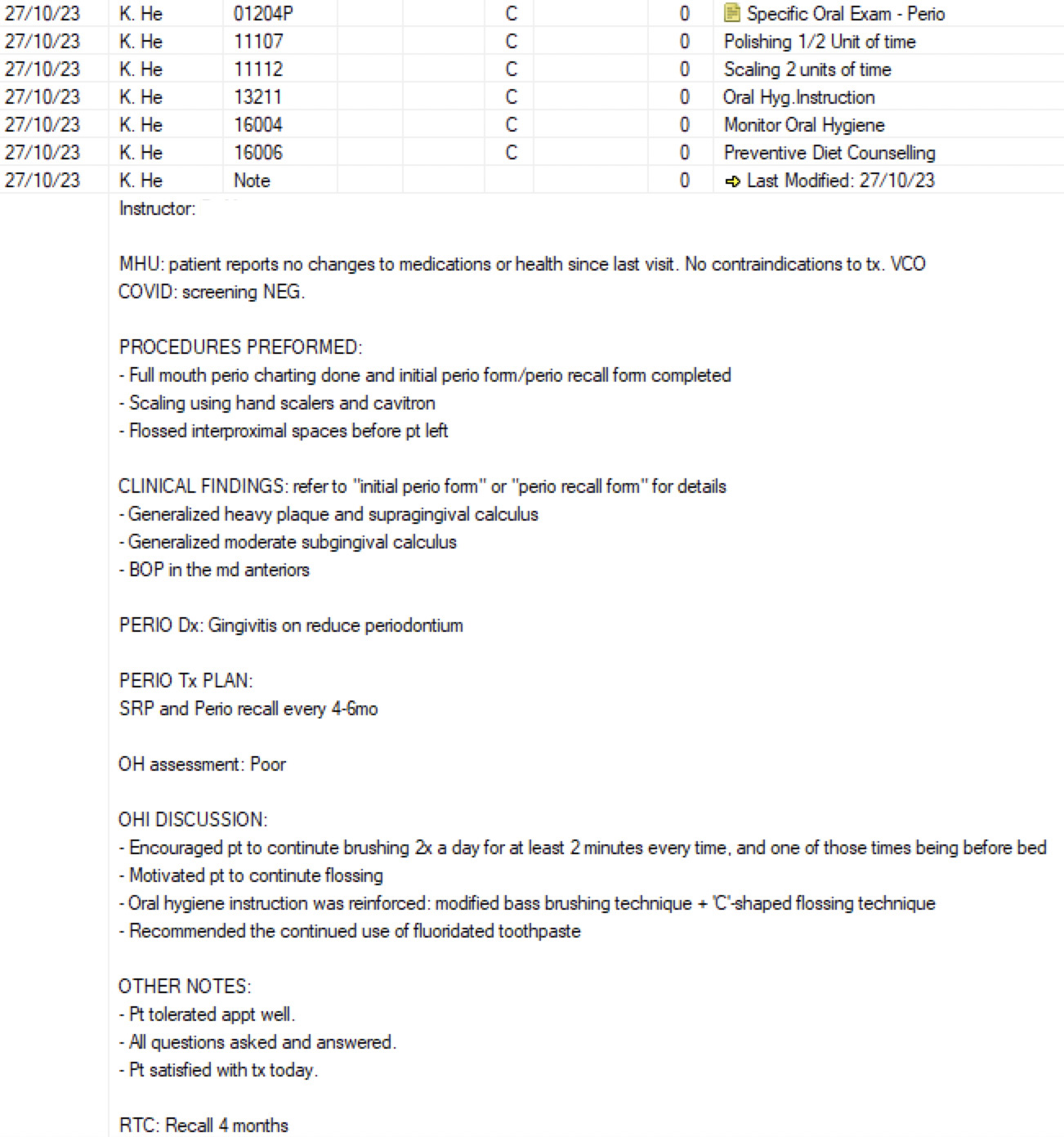
Note: “K. He” is my name. The instructor's name was removed to de-identify them. “C” stands for “Complete”. “MHU” stands for Medical History Update. “VCO” stands for Verbal Consent Obtained. “RTC” stands for Return to Clinic.
Appointment # 2 November 10, 2023
- Complete exam, including an extraoral and intraoral exam
- Planning of restorative treatment
- Risk analysis assessment
- Radiographs were taken according to As Low As Reasonably Achievable (ALARA) Principles and what was observed clinically. This included 4 bitewing images and 1 anterior periapical image.
- Oral hygiene was again reinforced using a hand mirror so the patient could visualize what thorough toothbrushing entailed (using the Modified Bass method). He could then relay this information to his PSW.
- The patient was provided an oral hygiene kit which included a soft-bristle toothbrush, gum stimulator, floss picks, and fluoridated toothpaste
- Reinforced dietary counselling
Official notes from the appointment:
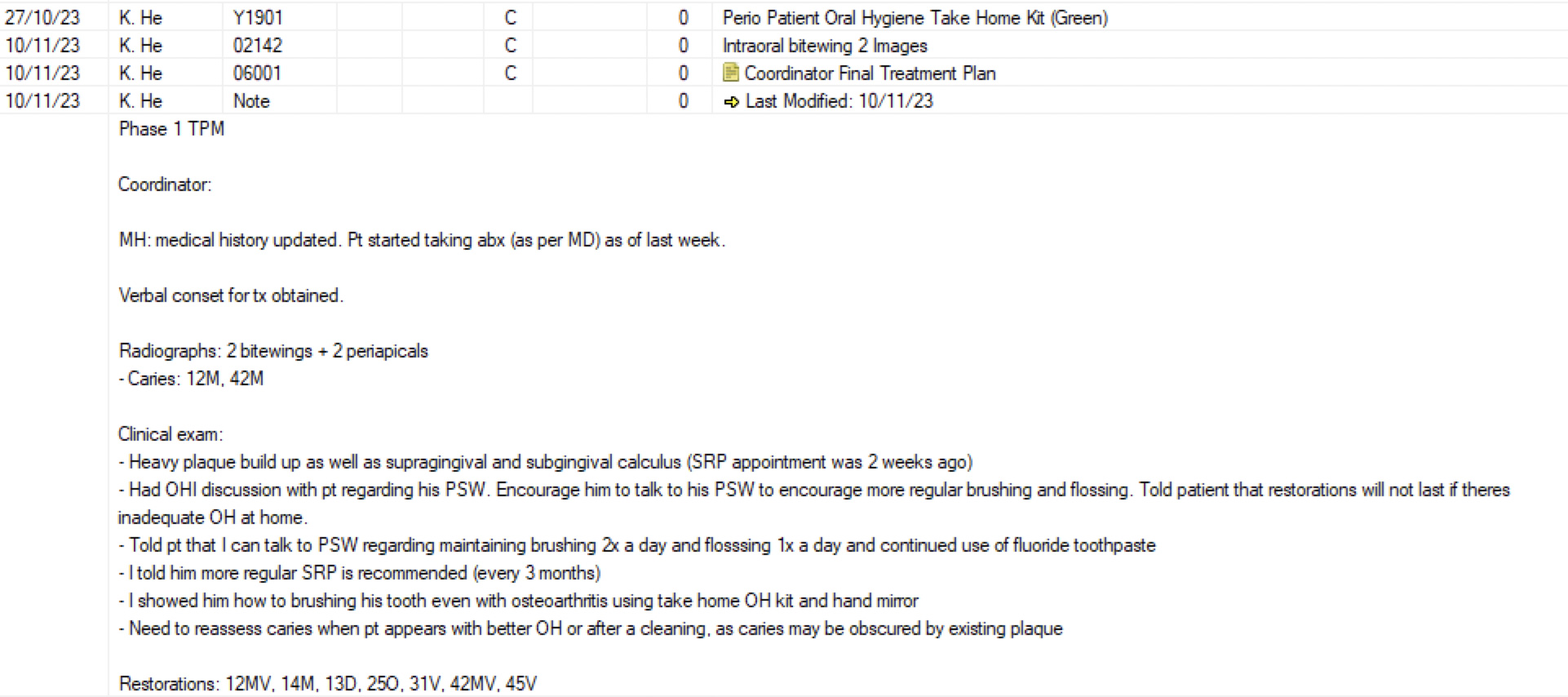
Note: “TPM” stands for “Treatment Planning”. The Coordinator’s name was removed to de-identify them.
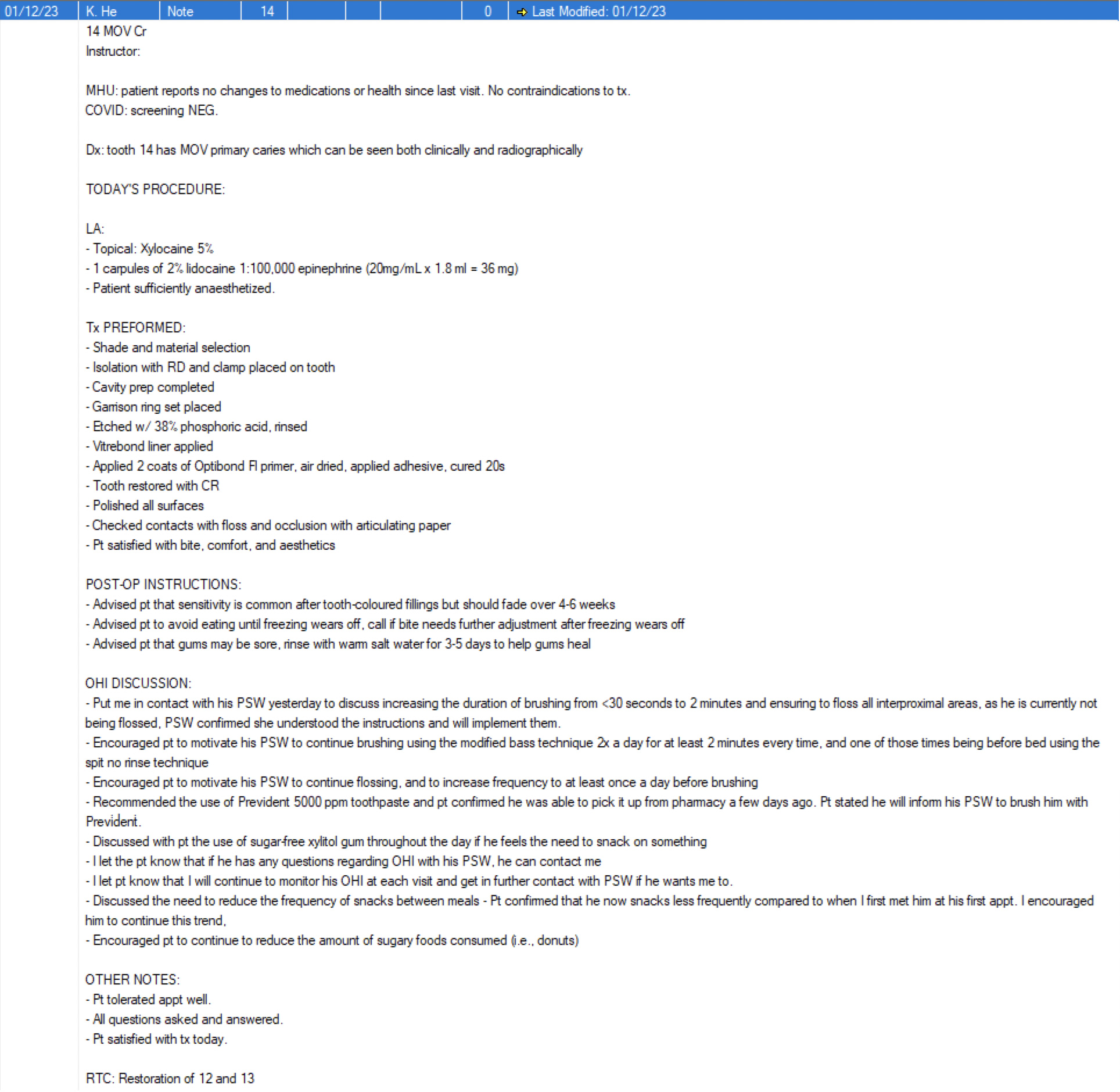
Appointment # 3 December 1, 2023
- Restoration of 14MOV with composite resin
- Monitor compliance to OHI
- OHI and diet counselling reinforcement (see notes below)
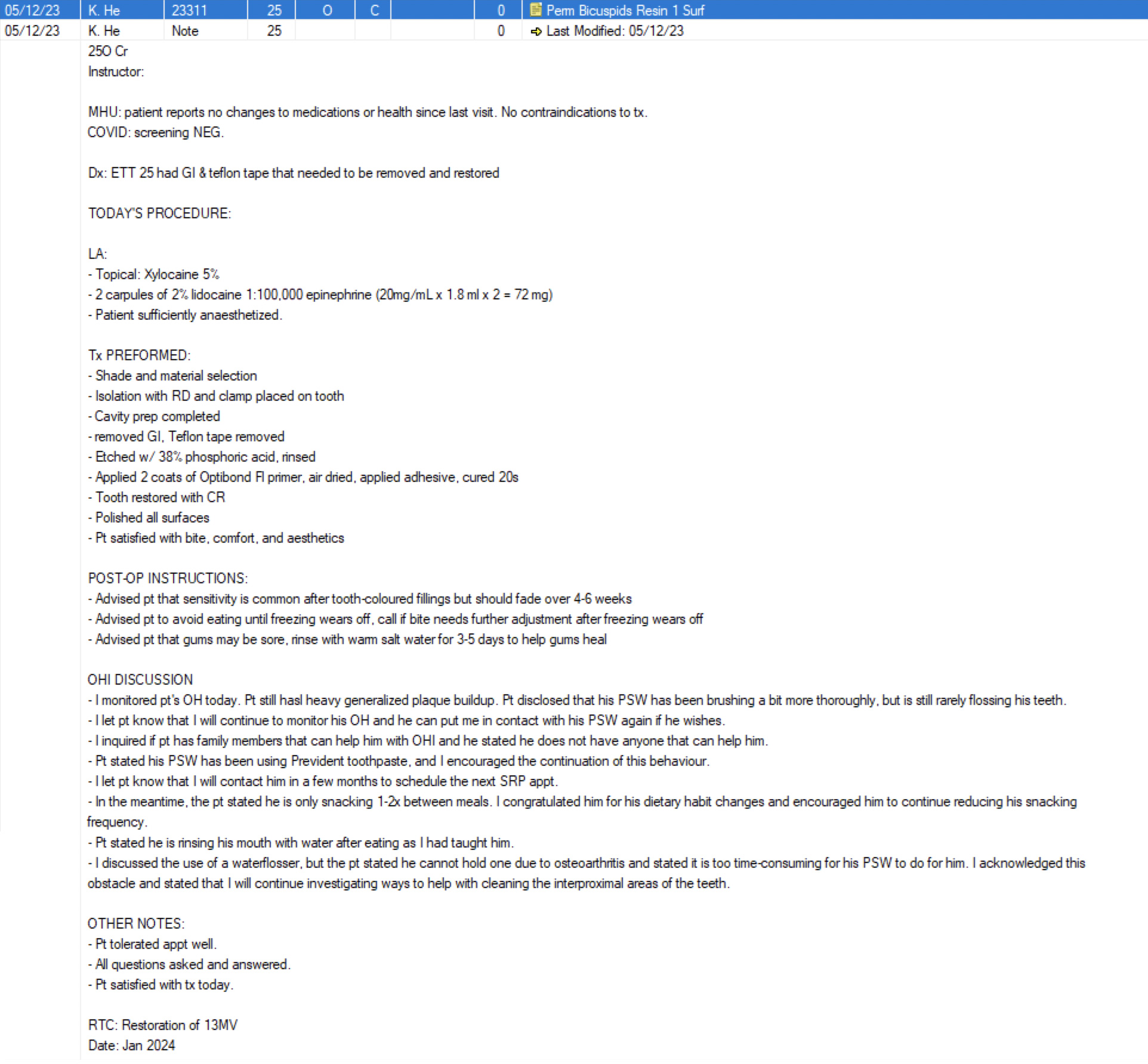
Appointment # 4 December 5, 2023
- Restoration of 25O with composite resin
- Monitor compliance to OHI
- OHI and diet counselling reinforcement (see notes below)
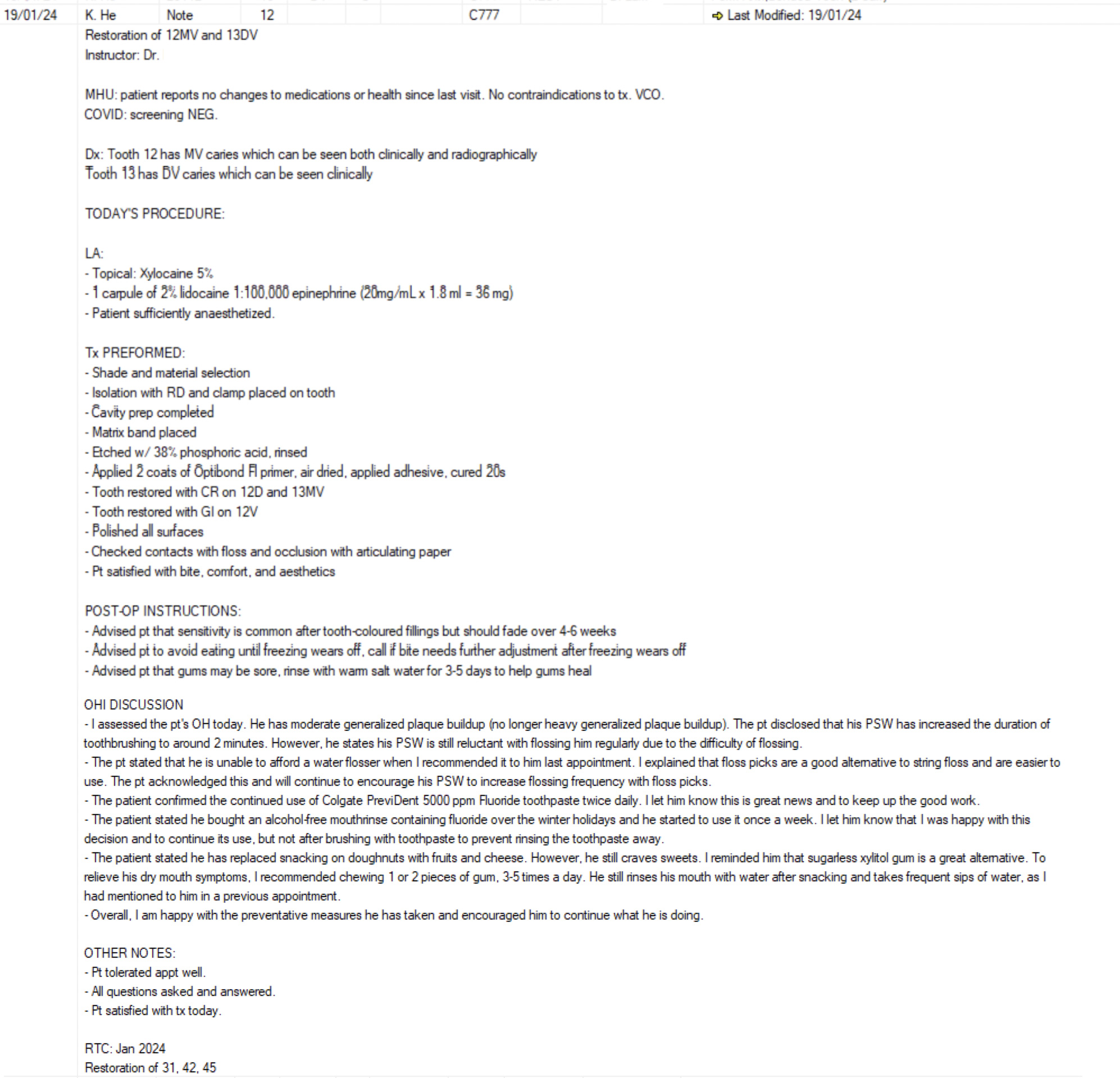
Appointment # 5 January 19, 2024
- Restoration of 12MV and 13DV with RMGI
- Monitor compliance to OHI
- OHI and diet counselling reinforcement (see notes below)
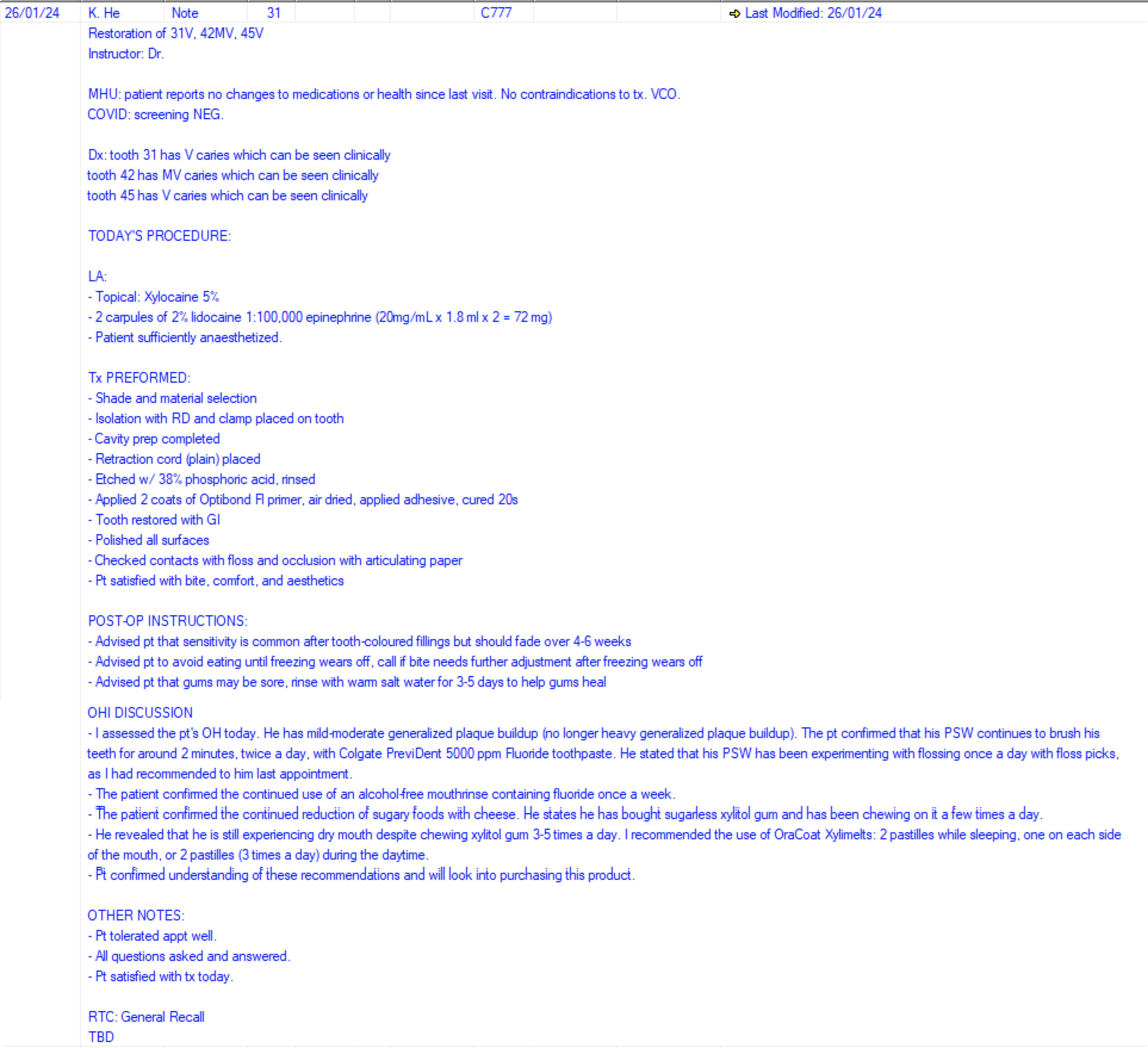
Appointment #6 January 26, 2024
- Restoration of 31V, 42MV and 45V with RMGI
- Monitor compliance to OHI
- OHI and diet counselling reinforcement (see notes below)
Summary of Oral Hygiene Instruction and Diet Counselling
Upon looking intraorally during the first appointment, it was evident that the patient’s at-home hygiene was inadequate. Thus, I demonstrated the Modified Bass method to him using a hand mirror so that he could encourage his PSW to brush his teeth using that method:
- Place the toothbrush at a 45-degree angle to the gums/li>
- Brush two to three teeth at a time using a circular motion/li>
- At the end of the circular motion, turn the toothbrush down the tooth, away from the gum line. Avoid aggressive horizontal scrubbing, as this may lead to gum recession and loss of tooth structure.4Warreth A. Dental Caries and Its Management. Int J Dent. 2023 Jan 3;2023:9365845. doi: 10.1155/2023/9365845. PMID: 36636170; PMCID: PMC9831703.,13Janakiram C, Varghese N, Venkitachalam R, Joseph J, Vineetha K. Comparison of modified Bass, Fones and normal tooth brushing technique for the efficacy of plaque control in young adults- A randomized clinical trial. J Clin Exp Dent. 2020 Feb 1;12(2):e123-e129. doi: 10.4317/jced.55747. PMID: 32071693; PMCID: PMC7018473./li>
- Brush all surfaces of the teeth in this manner
Toothpaste:
- I encouraged the use of the Colgate PreviDent 5000 ppm fluoride toothpaste, as he is at high caries risk. I taught him to use a pea-sized amount of this toothpaste for 2 minutes.11Weyant RJ, Tracy SL, Anselmo TT, Beltrán-Aguilar ED, Donly KJ, Frese WA, Hujoel PP, Iafolla T, Kohn W, Kumar J, Levy SM, Tinanoff N, Wright JT, Zero D, Aravamudhan K, Frantsve-Hawley J, Meyer DM; American Dental Association Council on Scientific Affairs Expert Panel on Topical Fluoride Caries Preventive Agents. Topical fluoride for caries prevention: executive summary of the updated clinical recommendations and supporting systematic review. J Am Dent Assoc. 2013 Nov;144(11):1279-91. doi: 10.14219/jada.archive.2013.0057. Erratum in: J Am Dent Assoc. 2013 Dec;144(12):1335. Dosage error in article text. PMID: 24177407; PMCID: PMC4581720.
- I reinforced the use of the spit-don’t-rinse method so that the fluoride can coat the teeth for a longer duration of time, as he initially stated that he rinses his mouth with water after being brushed11Weyant RJ, Tracy SL, Anselmo TT, Beltrán-Aguilar ED, Donly KJ, Frese WA, Hujoel PP, Iafolla T, Kohn W, Kumar J, Levy SM, Tinanoff N, Wright JT, Zero D, Aravamudhan K, Frantsve-Hawley J, Meyer DM; American Dental Association Council on Scientific Affairs Expert Panel on Topical Fluoride Caries Preventive Agents. Topical fluoride for caries prevention: executive summary of the updated clinical recommendations and supporting systematic review. J Am Dent Assoc. 2013 Nov;144(11):1279-91. doi: 10.14219/jada.archive.2013.0057. Erratum in: J Am Dent Assoc. 2013 Dec;144(12):1335. Dosage error in article text. PMID: 24177407; PMCID: PMC4581720.
Flossing:
- The patient discussed the difficulty of his PSW to floss his teeth. Thus, I encouraged the use of floss picks, as it is much easier to manoeuvre and can still remove plaque from the interproximal areas.
- I encouraged him to get flossed at least once a day before brushing using the “C”-shaped flossing technique, which can be done with a floss pick14Hujoel PP, Cunha-Cruz J, Banting DW, Loesche WJ. Dental flossing and interproximal caries: a systematic review. J Dent Res. 2006 Apr;85(4):298-305. doi: 10.1177/154405910608500404. PMID: 16567548.
Diet Counselling:
- I encouraged the patient to try sugar-free xylitol gum to increase saliva flow and to help buffer the pH of the mouth12Rethman MP, Beltrán-Aguilar ED, Billings RJ, Hujoel PP, Katz BP, Milgrom P, Sohn W, Stamm JW, Watson G, Wolff M, Wright JT, Zero D, Aravamudhan K, Frantsve-Hawley J, Meyer DM; American Dental Association Council on Scientific Affairs Expert Panel on Nonfluoride Caries-Preventive Agents. Nonfluoride caries-preventive agents: executive summary of evidence-based clinical recommendations. J Am Dent Assoc. 2011 Sep;142(9):1065-1071. doi: 10.14219/jada.archive.2011.0329. PMID: 21987836.
- I encouraged the patient to decrease his snacking frequency in between meals to reduce the frequency of acid attacks on his teeth. After snacking, I explained the importance of rinsing the mouth with water
- I recommended the consumption of less cariogenic foods, such as cheese, rather than sugary baked goods, like doughnuts7Tungare S, Paranjpe AG. Diet and Nutrition to Prevent Dental Problems. [Updated 2023 Jul 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534248/
Speaking with the PSW:
- Unfortunately, the patient revealed that his PSW was reluctant to take on more thorough oral hygiene techniques. He requested that I speak with his PSW.
- The patient put me on the phone with his PSW one day, and I had a discussion regarding the importance of oral hygiene and the adverse effects of inadequate oral hygiene on his overall health. I discussed how we can gradually improve his oral hygiene over time rather than all at once if the PSW felt uncomfortable with the steep learning curve.
- The PSW acknowledged these concerns and stated they would try their best. We decided to increase toothbrushing duration from less than 30 seconds to 2 minutes. We also decided to floss every interproximal surface at least 4 times a week rather than 1-2 times a week. This will be increased as the PSW gains more confidence with the oral hygiene techniques.
Maintenance Treatment Plan
- Encourage regular SRP every 4 months and periodontal/general recall every 4 months. Radiographs (i.e., bitewings) should be taken every year (or earlier if suspected caries or pathology) to assess for new caries or recurrent caries. This is based on the recommendations by the American Dental Associaton’s “Dental Radiographic Examinations: Recommendations for Patient Selection and Limiting Radiation Exposure”16American Dental Association (2012). Dental Radiographic Examinations: Recommendations for Patient Selection and Limiting Radiation Exposure. and ALARA principles. If incipient lesions are found, they are to be monitored closely and preventative measures employed as soon as possible (i.e., fluoride treatment).
- Check oral hygiene and reinforce OHI/diet counselling at every appointment. Monitor dietary changes in the long term. Monitor changes to systemic health, such as the addition of any medications that may cause xerostomia and advise of salivary substitutes as necessary.7Tungare S, Paranjpe AG. Diet and Nutrition to Prevent Dental Problems. [Updated 2023 Jul 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534248/,8Janakiram C, Deepan Kumar CV, Joseph J. Xylitol in preventing dental caries: A systematic review and meta-analyses. J Nat Sci Biol Med. 2017 Jan-Jun;8(1):16-21. doi: 10.4103/0976-9668.198344. PMID: 28250669; PMCID: PMC5320817.,9Mickenautsch S, Leal SC, Yengopal V, Bezerra AC, Cruvinel V. Sugar-free chewing gum and dental caries: a systematic review. J Appl Oral Sci. 2007 Apr;15(2):83-8. doi: 10.1590/s1678-77572007000200002. PMID: 19089107; PMCID: PMC4327235.
- New risk assessment every 4 months to monitor compliance and encourage continuation of progress. Watch for new risk factors and reduce them when possible.
Treatment Outcomes
When all the treatments were complete, the patient stated his teeth no longer regularly felt “sticky” and that his oral health had improved. His gingiva appeared less inflamed than when I did his first initial periodontal exam. There was less plaque and calculus accumulation. All the carious lesions were removed and filled with composite resin/RMGI. Preventative measures, including OHI and diet counselling, were reinforced at each appointment to ensure compliance and monitoring, as detailed in the notes of each appointment.
To summarize the preventative measures taken, the patient, along with his PSW, was able to:
- Increase brushing frequency to twice a day with the Modified Bass technique
- Increase brushing duration from less than 30 seconds to 2 minutes
- Use Colgate PreviDent 5000 ppm fluoride toothpaste twice a day using the spit-don’t-rinse method15Talwar M, Borzabadi-Farahani A, Lynch E, Borsboom P, Ruben J. Remineralization of Demineralized Enamel and Dentine Using 3 Dentifrices-An InVitro Study. Dent J (Basel). 2019 Sep 2;7(3):91. doi: 10.3390/dj7030091. PMID: 31480726; PMCID: PMC6784461.
- Increase the frequency of flossing to at least 4 times a week
- Reduce the frequency of snacking
- Replace the consumption of sugary foods/beverages to less cariogenic foods/beverages
- Increase the frequency of seeing the dentist to monitor for compliance, presence of new active disease, and receive preventative care (i.e., SRP)
- Incorporate xylitol-containing gum into his diet to increase salivary flow and reduce caries risk
- Increase motivation to seek regular dental care
In conclusion, he stated he will continue to employ these preventative measures to reduce his risk of disease. He demonstrated a very thorough understanding of how caries and periodontal disease develop by the end of the second appointment and is doing his part to prevent active disease. I will continue to see him at least once every 4 months to monitor his oral health and continue to provide preventative services until I graduate in 2025. This includes scaling and root planing, polishing, fluoride varnish application, and restoration of any new carious lesions. I am very grateful for this experience, as I learned how to provide care to someone with such a complex medical/dental/social history, and educate him on the preventative concepts that were taught at school. Learning how to adapt to patients with musculoskeletal conditions also taught me resilience, as it took a lot of trial-and-error to find the appropriate position for me to provide dental care to him in a wheelchair and think outside the box to identify the best at-home hygiene routine for the patient. Despite having to stand up to perform dentistry, I am pleased with the outcomes and the patient was satisfied with all his cavities being treated.
References
- 1.Lamont T, Worthington HV, Clarkson JE, Beirne PV. Routine scale and polish for periodontal health in adults. Cochrane Database Syst Rev. 2018 Dec 27;12(12):CD004625. doi: 10.1002/14651858.CD004625.pub5. PMID: 30590875; PMCID: PMC6516960.
- 2.Medjedovic E, Medjedovic S, Deljo D, Sukalo A. IMPACT OF FLUORIDE ON DENTAL HEALTH QUALITY. Mater Sociomed. 2015 Dec;27(6):395-8. doi: 10.5455/msm.2015.27.395-398. PMID: 26889098; PMCID: PMC4733546
- 3.Nassar Y, Brizuela M. The Role of Fluoride on Caries Prevention. [Updated 2023 Mar 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK587342/
- 4.Warreth A. Dental Caries and Its Management. Int J Dent. 2023 Jan 3;2023:9365845. doi: 10.1155/2023/9365845. PMID: 36636170; PMCID: PMC9831703.
- 5.American Dental Association (2023). Evidence-Based Clinical Practice Guideline on Restorative Treatments for Caries Lesions: A Report from the American Dental Association.
- 6.Dhar V, Pilcher L, Fontana M, González-Cabezas C, Keels MA, Mascarenhas AK, Nascimento M, Platt JA, Sabino GJ, Slayton R, Tinanoff N, Young DA, Zero DT, Pahlke S, Urquhart O, O'Brien KK, Carrasco-Labra A. Evidence-based clinical practice guideline on restorative treatments for caries lesions: A report from the American Dental Association. J Am Dent Assoc. 2023 Jul;154(7):551-566.e51. doi: 10.1016/j.adaj.2023.04.011. PMID: 37380250.
- 7.Tungare S, Paranjpe AG. Diet and Nutrition to Prevent Dental Problems. [Updated 2023 Jul 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534248/
- 8.Janakiram C, Deepan Kumar CV, Joseph J. Xylitol in preventing dental caries: A systematic review and meta-analyses. J Nat Sci Biol Med. 2017 Jan-Jun;8(1):16-21. doi: 10.4103/0976-9668.198344. PMID: 28250669; PMCID: PMC5320817.
- 9.Mickenautsch S, Leal SC, Yengopal V, Bezerra AC, Cruvinel V. Sugar-free chewing gum and dental caries: a systematic review. J Appl Oral Sci. 2007 Apr;15(2):83-8. doi: 10.1590/s1678-77572007000200002. PMID: 19089107; PMCID: PMC4327235.
- 10.Smiley CJ, Tracy SL, Abt E, Michalowicz BS, John MT, Gunsolley J, Cobb CM, Rossmann J, Harrel SK, Forrest JL, Hujoel PP, Noraian KW, Greenwell H, Frantsve-Hawley J, Estrich C, Hanson N. Evidence-based clinical practice guideline on the nonsurgical treatment of chronic periodontitis by means of scaling and root planing with or without adjuncts. J Am Dent Assoc. 2015 Jul;146(7):525-35. doi: 10.1016/j.adaj.2015.01.026. PMID: 26113100.
- 11.Weyant RJ, Tracy SL, Anselmo TT, Beltrán-Aguilar ED, Donly KJ, Frese WA, Hujoel PP, Iafolla T, Kohn W, Kumar J, Levy SM, Tinanoff N, Wright JT, Zero D, Aravamudhan K, Frantsve-Hawley J, Meyer DM; American Dental Association Council on Scientific Affairs Expert Panel on Topical Fluoride Caries Preventive Agents. Topical fluoride for caries prevention: executive summary of the updated clinical recommendations and supporting systematic review. J Am Dent Assoc. 2013 Nov;144(11):1279-91. doi: 10.14219/jada.archive.2013.0057. Erratum in: J Am Dent Assoc. 2013 Dec;144(12):1335. Dosage error in article text. PMID: 24177407; PMCID: PMC4581720.
- 12.Rethman MP, Beltrán-Aguilar ED, Billings RJ, Hujoel PP, Katz BP, Milgrom P, Sohn W, Stamm JW, Watson G, Wolff M, Wright JT, Zero D, Aravamudhan K, Frantsve-Hawley J, Meyer DM; American Dental Association Council on Scientific Affairs Expert Panel on Nonfluoride Caries-Preventive Agents. Nonfluoride caries-preventive agents: executive summary of evidence-based clinical recommendations. J Am Dent Assoc. 2011 Sep;142(9):1065-1071. doi: 10.14219/jada.archive.2011.0329. PMID: 21987836.
- 13.Janakiram C, Varghese N, Venkitachalam R, Joseph J, Vineetha K. Comparison of modified Bass, Fones and normal tooth brushing technique for the efficacy of plaque control in young adults- A randomized clinical trial. J Clin Exp Dent. 2020 Feb 1;12(2):e123-e129. doi: 10.4317/jced.55747. PMID: 32071693; PMCID: PMC7018473.
- 14.Hujoel PP, Cunha-Cruz J, Banting DW, Loesche WJ. Dental flossing and interproximal caries: a systematic review. J Dent Res. 2006 Apr;85(4):298-305. doi: 10.1177/154405910608500404. PMID: 16567548.
- 15.Talwar M, Borzabadi-Farahani A, Lynch E, Borsboom P, Ruben J. Remineralization of Demineralized Enamel and Dentine Using 3 Dentifrices-An InVitro Study. Dent J (Basel). 2019 Sep 2;7(3):91. doi: 10.3390/dj7030091. PMID: 31480726; PMCID: PMC6784461.
- 16.American Dental Association (2012). Dental Radiographic Examinations: Recommendations for Patient Selection and Limiting Radiation Exposure.